This document discusses abscesses, including:
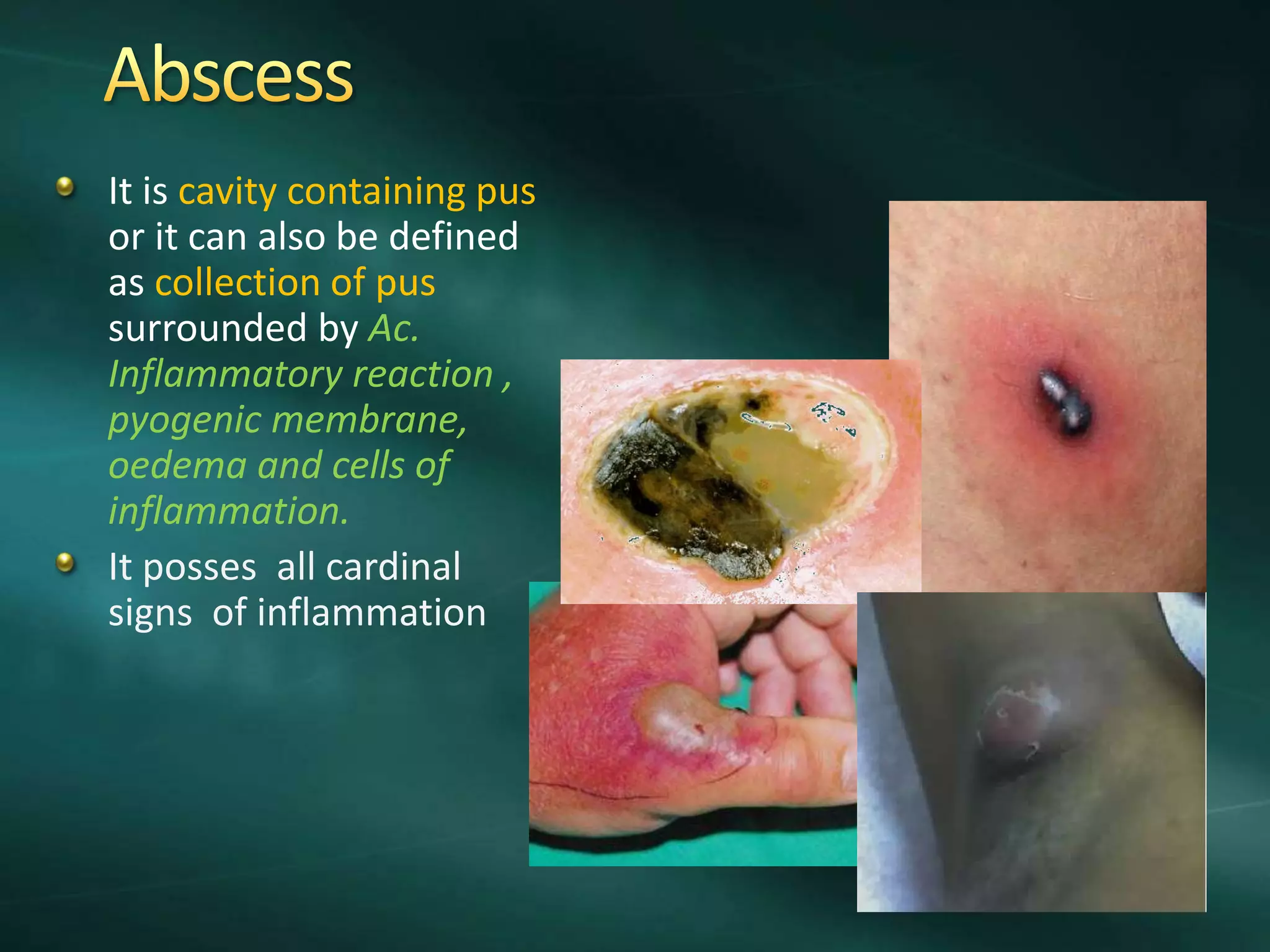
1. An abscess is a collection of pus surrounded by inflamed tissues and contains dead and dying white blood cells and bacteria.
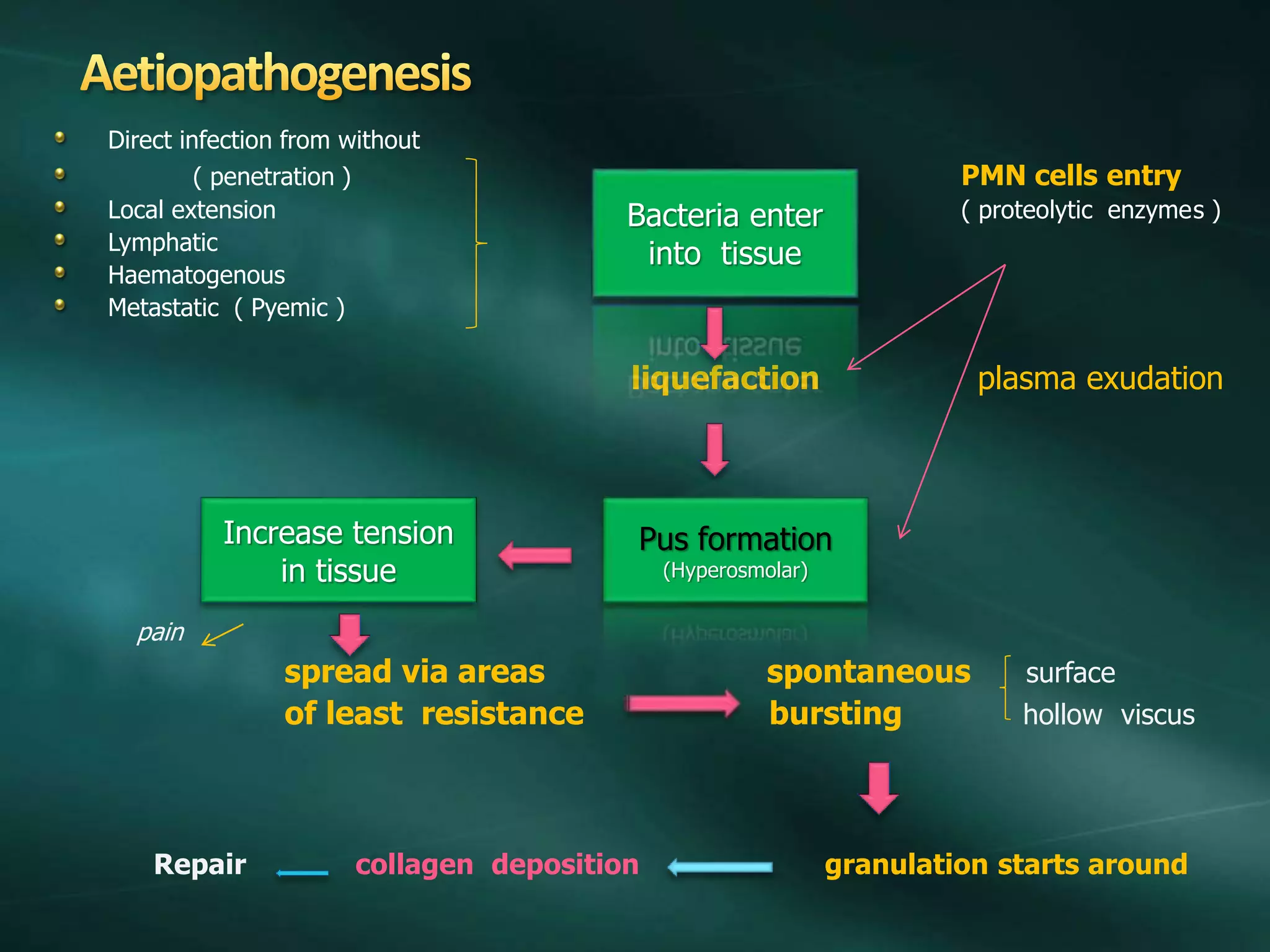
2. Abscesses spread along paths of least resistance and increase pressure, causing pain. They eventually burst spontaneously or require incision and drainage.
3. Treatment involves rest, elevation, antibiotics, and incision and drainage surgery to fully open and curette the abscess cavity.