This document discusses healthcare construction and facility design for safer environments and quality care. It covers several topics:
1. The roles of medical professionals, architects, researchers, and administrators in hospital design based on their knowledge and experience to reduce risks and spur innovation.
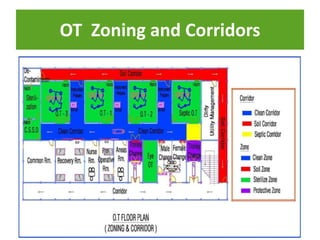
2. Key considerations in planning and designing different areas of a hospital like intensive care units, operating theaters, and diagnostic radiology departments to promote patient and staff safety, infection control, and quality care delivery.
3. International standards and regulations from organizations like WHO, JCI, and national building codes that provide guidelines for ventilation, sanitation, traffic flow, and other design elements.
4. The planning process from preliminary surveys to conceptual design,










































































































![4._LAY_OUT_OF_CRITICAL_CARE_UNIT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/4-250506110215-46b0d8f2-thumbnail.jpg?width=640&height=640&fit=bounds)










































