


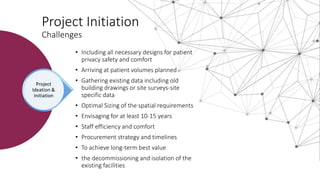
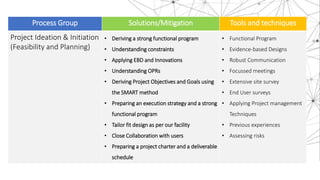





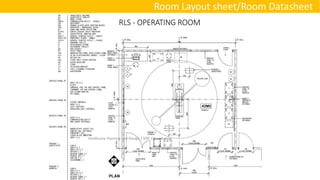
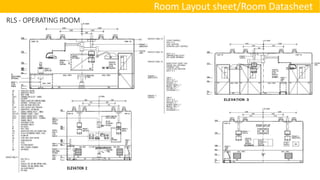

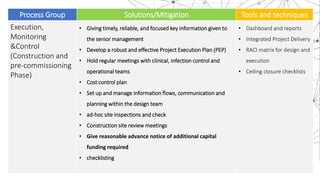


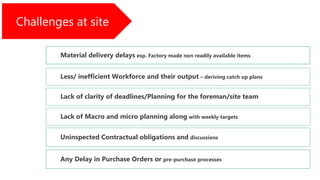



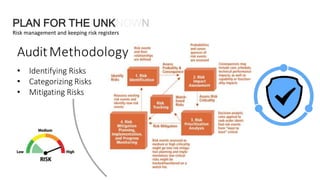



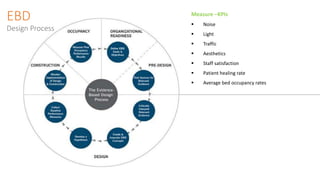

Healthcare construction renovations present unique challenges including safety concerns, technical challenges, and budgetary constraints. Extensive planning is required at the project initiation phase to properly envision space needs and operational requirements over the long term. Detailed design then requires generating site-specific drawings with input from user groups to streamline the design. Throughout the execution, monitoring, and control phase, regular progress reporting and risk assessment is important to ensure objectives are achieved on time and on budget while maintaining safety and compliance.



































































