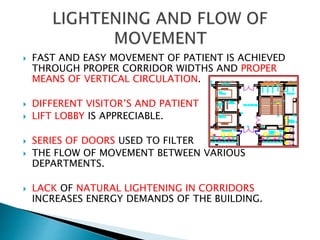
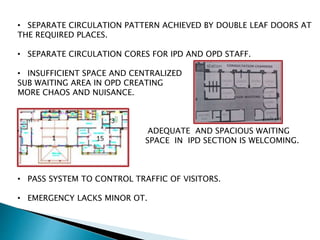
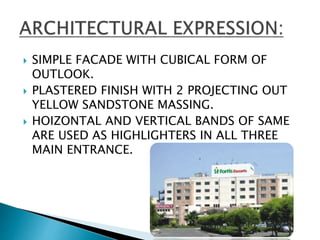
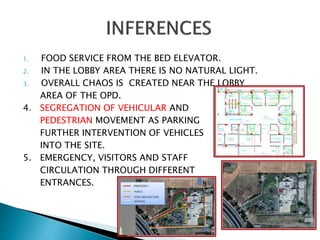
Hospitals are complex buildings with a wide range of services and functional units including diagnostic, treatment, hospitality, and inpatient care functions. Hospital design must consider efficiency, flexibility, interior design, aesthetics, accessibility, and cleanliness. The document discusses the layout and design considerations for key areas within a hospital including the emergency department, surgical department, intensive care unit, and patient care areas. Design should focus on optimal relationships and flow between departments to serve patients' needs.