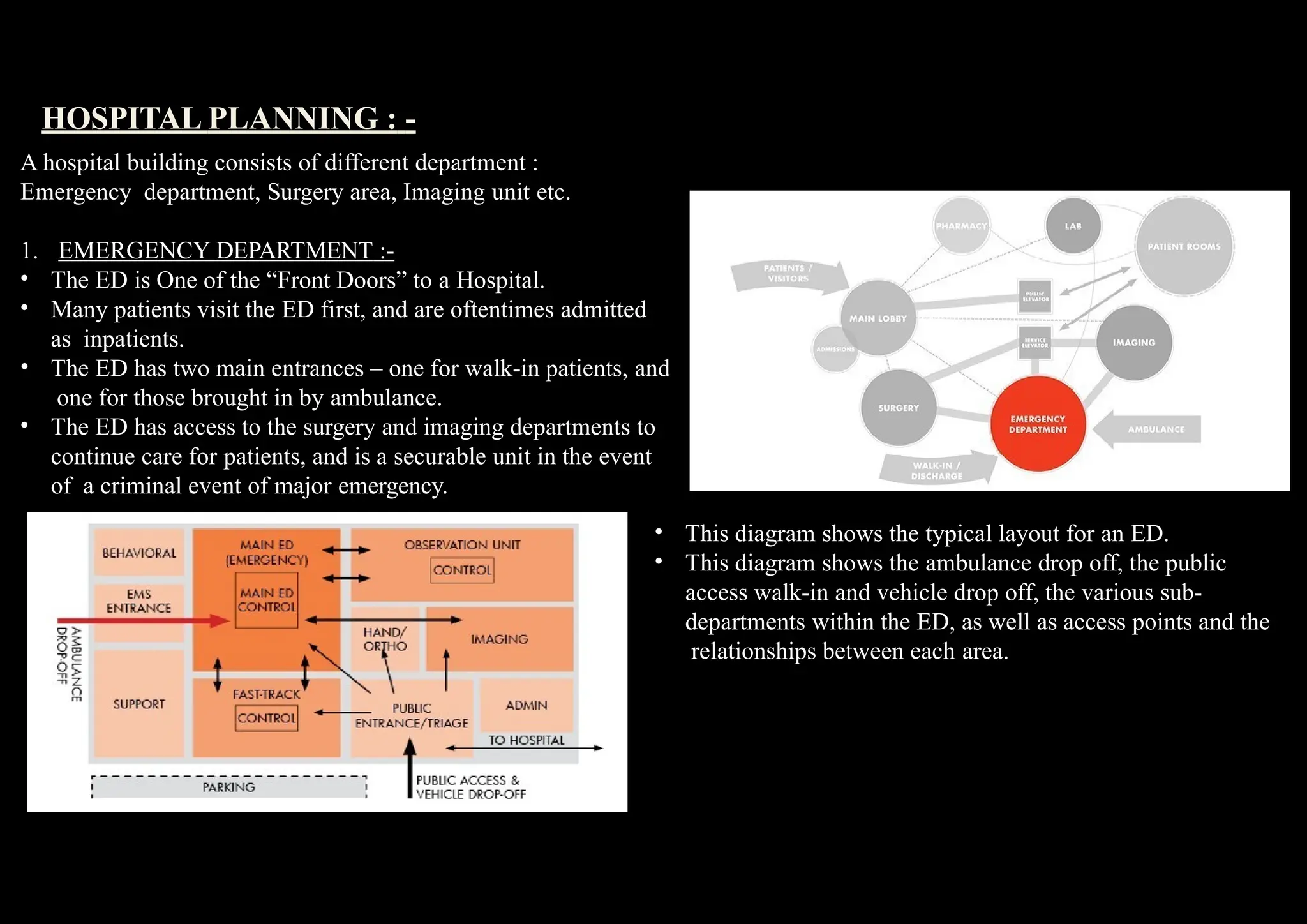
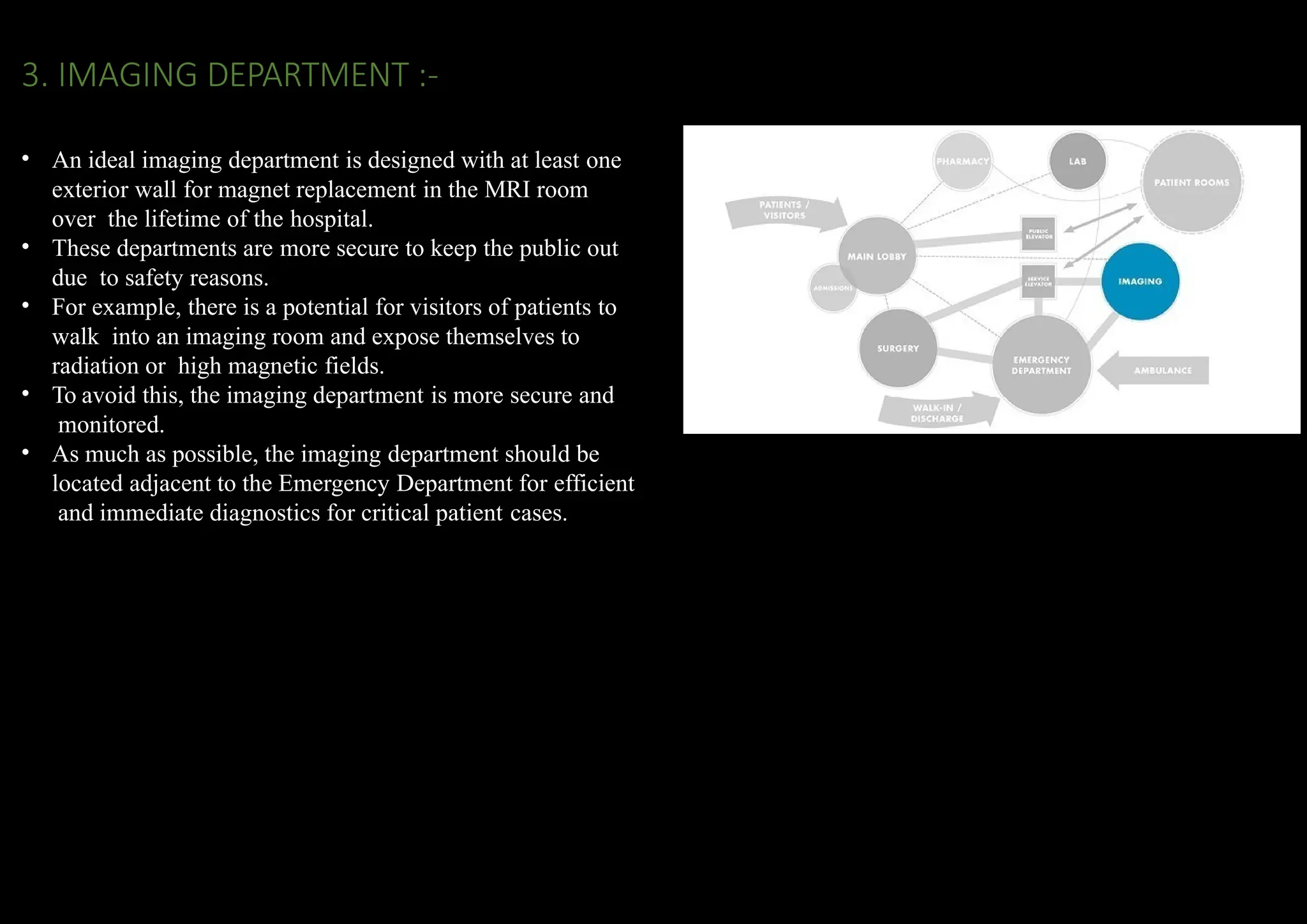
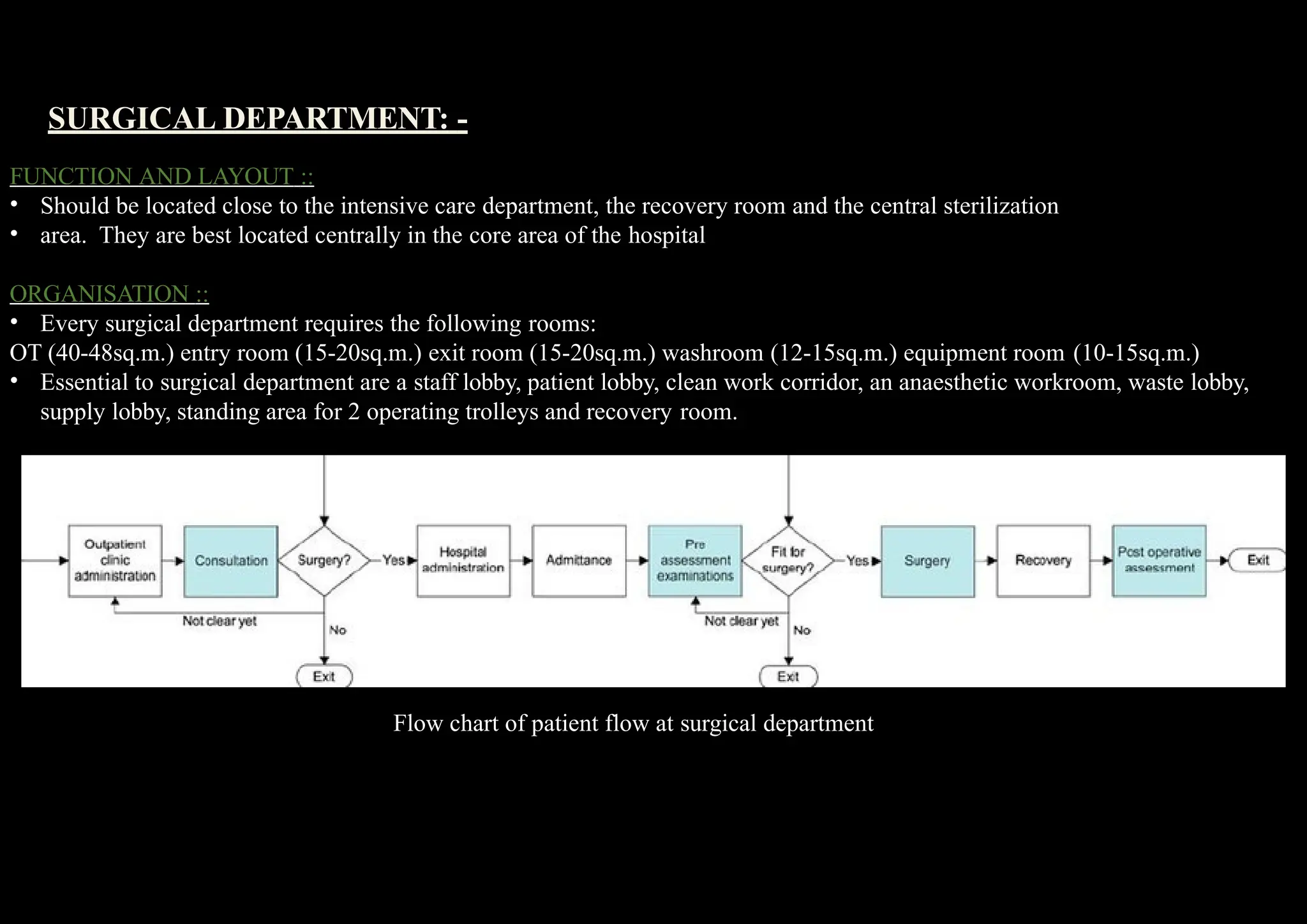
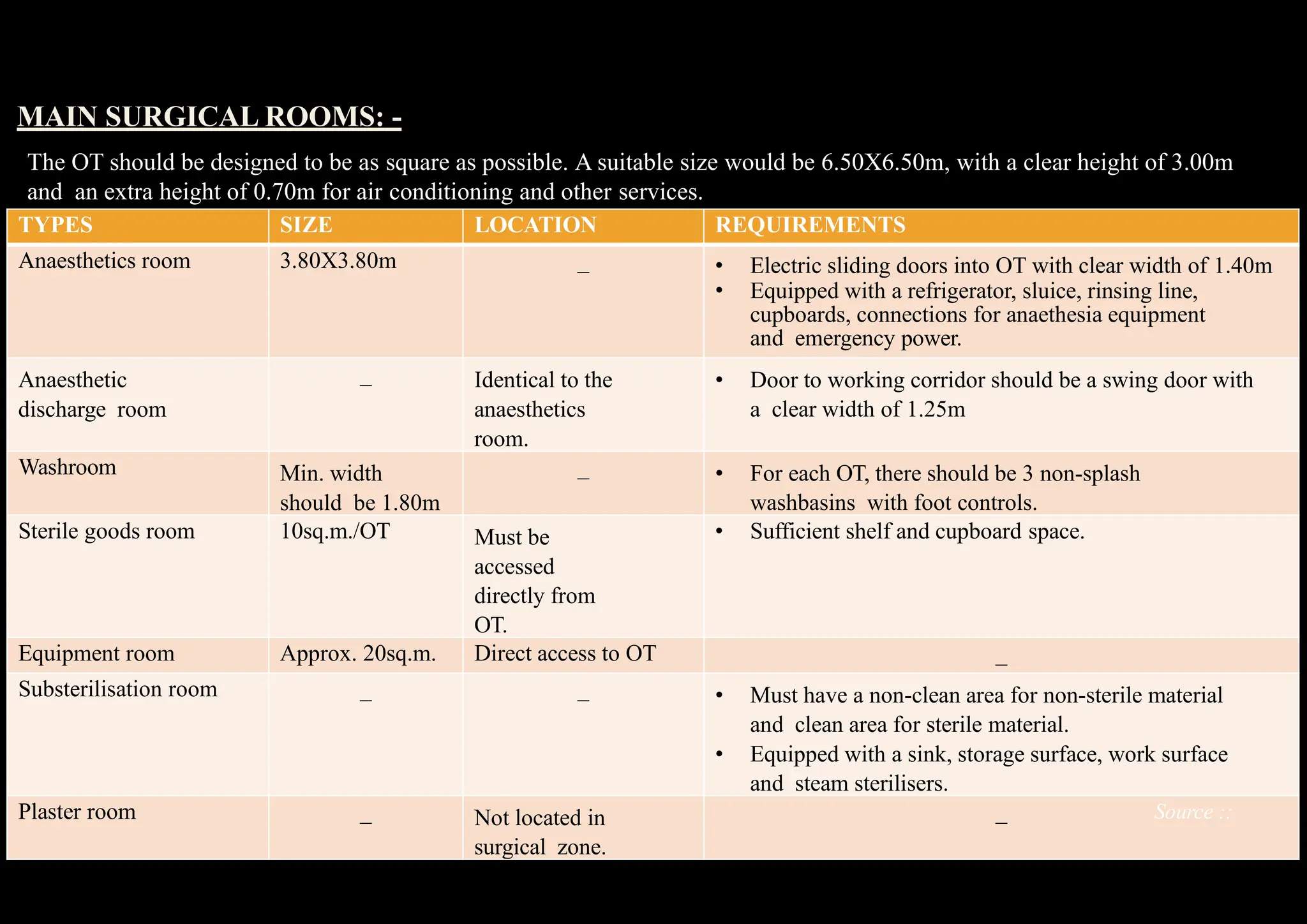
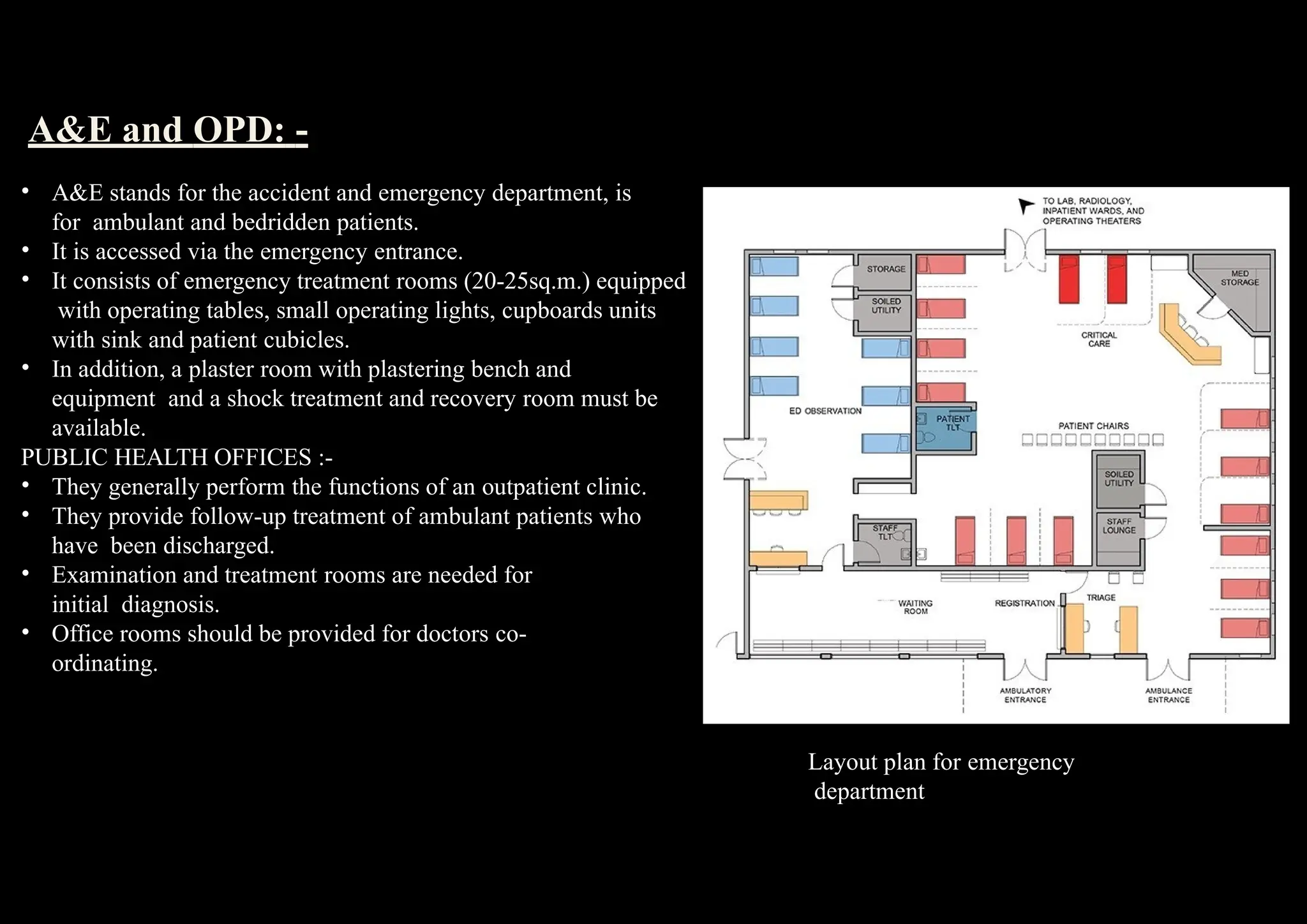
The document provides a comprehensive overview of hospital introduction, history, types, components, planning considerations, design considerations, and layout specifics for various departments. It categorizes hospitals based on functionality, size, location, and ownership, while outlining essential management systems like patient management and facility management. Additionally, it discusses key design aspects, such as creating a therapeutic environment, accessibility, security, and sustainable practices, along with detailed spatial requirements for critical areas like emergency, surgical, and imaging departments.