Download as PPSX, PPTX

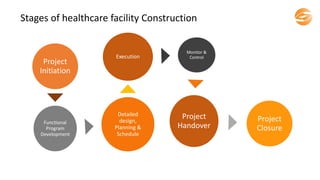

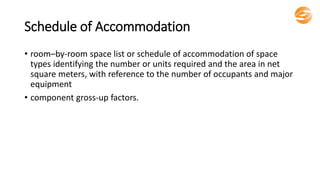
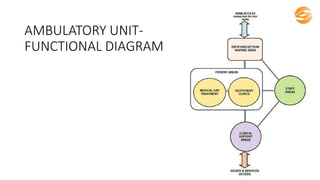
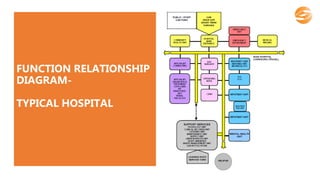

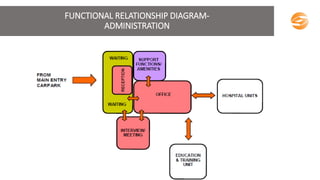
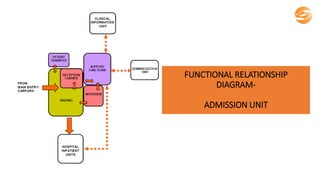
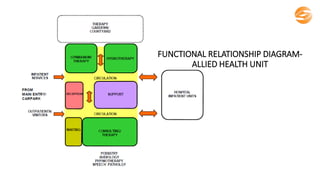
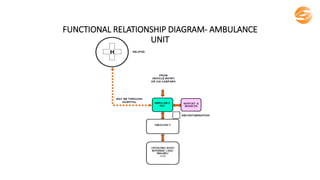
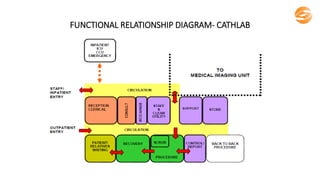
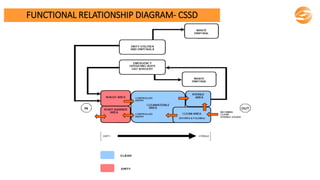
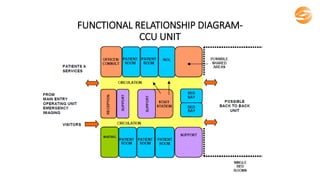
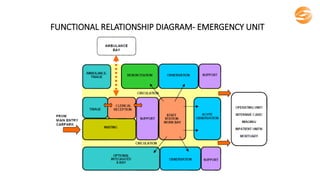
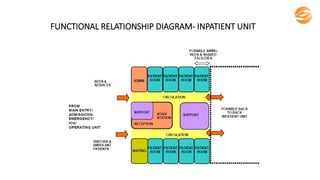
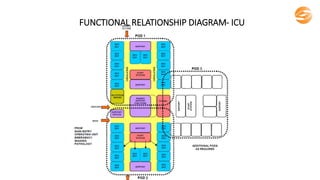
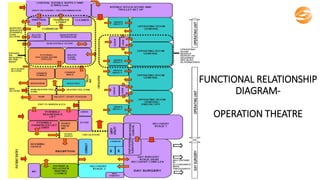
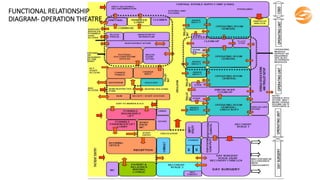
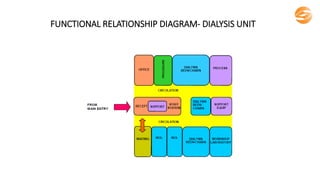
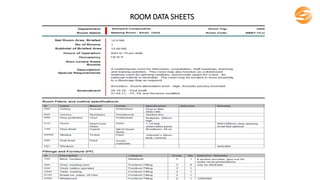
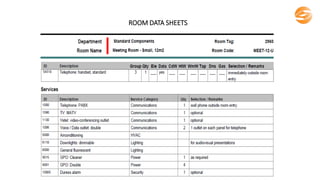
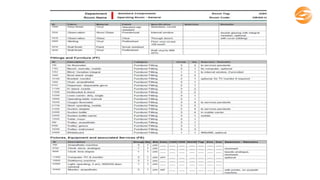
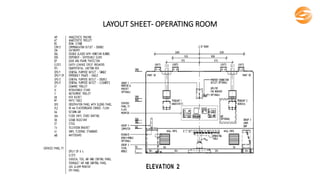
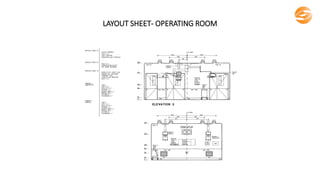
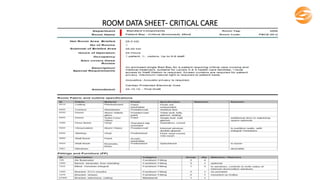
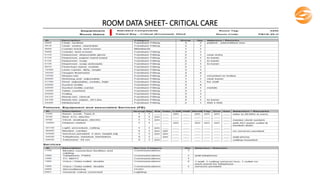
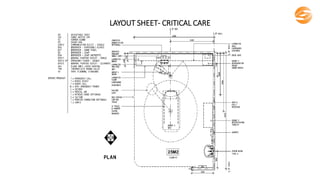
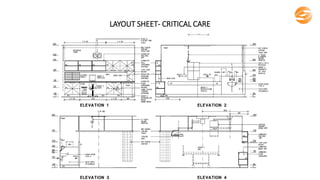


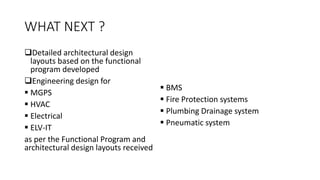
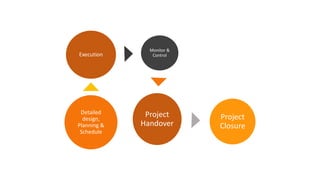





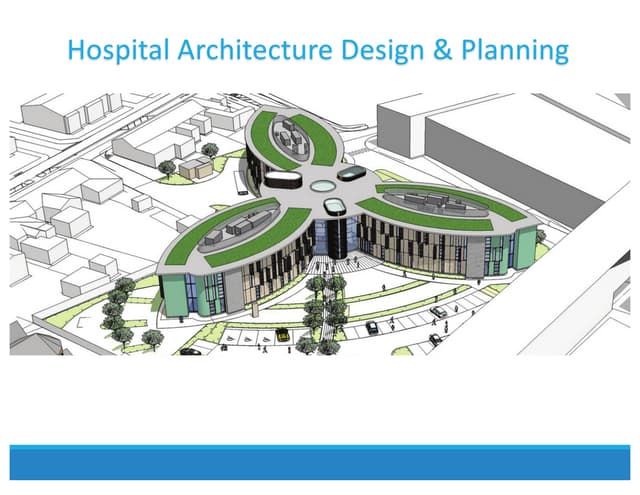
The document outlines the stages and essential components of healthcare facility design and construction, emphasizing the importance of a functional program that details operational needs and relationships between various components within the facility. It highlights key planning parameters, activities, workload projections, and the design criteria necessary for effective healthcare facility management. Additionally, it showcases services offered by STAT Consultancy, including project feasibility studies, facility planning, and project management, and notes their experience in successfully completing over 40 projects in India and the GCC.





























































![4._LAY_OUT_OF_CRITICAL_CARE_UNIT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/4-250506110215-46b0d8f2-thumbnail.jpg?width=640&height=640&fit=bounds)




![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)


![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)













