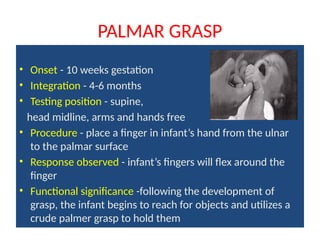
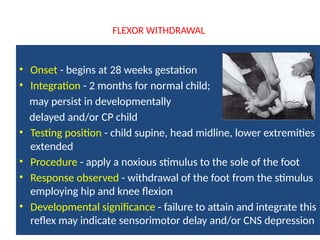
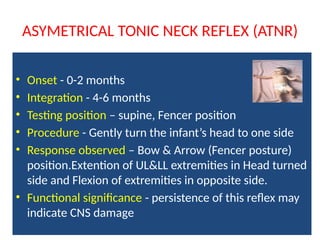
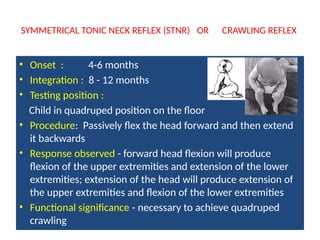
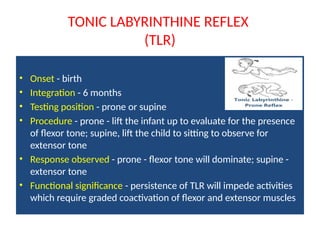
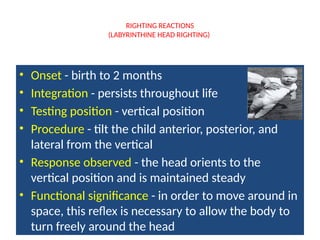
The document outlines various primitive reflexes essential for protection and survival in infants, detailing their onset, integration, testing positions, and functional significance. It emphasizes the importance of reflex testing for therapists to diagnose developmental delays or conditions and tailor interventions. Each reflex, such as the rooting and sucking reflexes, has specific developmental milestones and implications for physical and neural health.