BASIC COMPONENT OF
MOTORDEVELOPMENT
There are four basic component
Head control
Increased extensor control
Developing rotatory components
Equilibrium reactions
3.
HIGHER LEVEL MOVEMENTS
Asthe head rights extensor tone develops in upper limb and child
assumes the prone-on-elbow---to extend elbows---quadruped and
finally reciprocal creeping
Both flexor and extensor tone is developed to produce coordinated
movements
4.
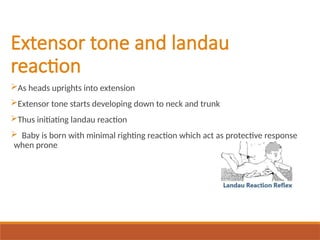
Extensor tone andlandau
reaction
As heads uprights into extension
Extensor tone starts developing down to neck and trunk
Thus initiating landau reaction
Baby is born with minimal righting reaction which act as protective response
when prone
6.
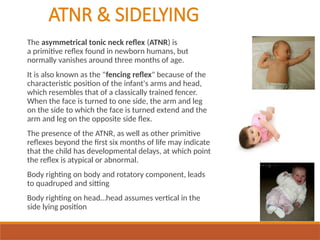
ATNR & SIDELYING
Theasymmetrical tonic neck reflex (ATNR) is
a primitive reflex found in newborn humans, but
normally vanishes around three months of age.
It is also known as the "fencing reflex" because of the
characteristic position of the infant's arms and head,
which resembles that of a classically trained fencer.
When the face is turned to one side, the arm and leg
on the side to which the face is turned extend and the
arm and leg on the opposite side flex.
The presence of the ATNR, as well as other primitive
reflexes beyond the first six months of life may indicate
that the child has developmental delays, at which point
the reflex is atypical or abnormal.
Body righting on body and rotatory component, leads
to quadruped and sitting
Body righting on head…head assumes vertical in the
side lying position
7.
STNR
Symmetrical tonic neckreflex (STNR) is a bridging or transitional
brainstem reflex that is not a primitive reflex but is an important
developmental stage and is necessary for a baby for transition from
lying on the floor quadruped crawling or creeping.
Onset of STNR occurs between 4–6 months and its integration occurs by
8–12 months.
It allows babies to make the transition from laying down to getting up
on their hands and knees.
8.
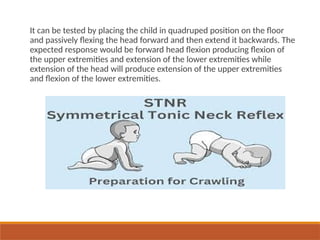
It can betested by placing the child in quadruped position on the floor
and passively flexing the head forward and then extend it backwards. The
expected response would be forward head flexion producing flexion of
the upper extremities and extension of the lower extremities while
extension of the head will produce extension of the upper extremities
and flexion of the lower extremities.
9.
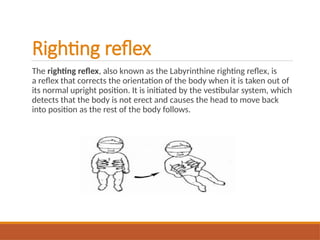
Righting reflex
The rightingreflex, also known as the Labyrinthine righting reflex, is
a reflex that corrects the orientation of the body when it is taken out of
its normal upright position. It is initiated by the vestibular system, which
detects that the body is not erect and causes the head to move back
into position as the rest of the body follows.
10.
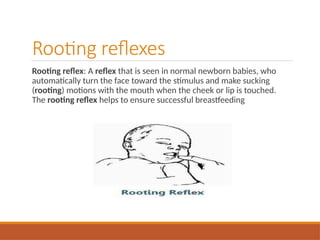
Rooting reflexes
Rooting reflex:A reflex that is seen in normal newborn babies, who
automatically turn the face toward the stimulus and make sucking
(rooting) motions with the mouth when the cheek or lip is touched.
The rooting reflex helps to ensure successful breastfeeding
11.
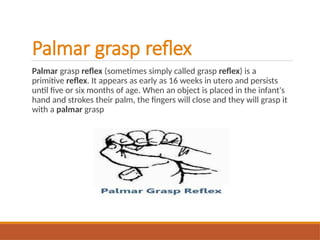
Palmar grasp reflex
Palmargrasp reflex (sometimes simply called grasp reflex) is a
primitive reflex. It appears as early as 16 weeks in utero and persists
until five or six months of age. When an object is placed in the infant's
hand and strokes their palm, the fingers will close and they will grasp it
with a palmar grasp
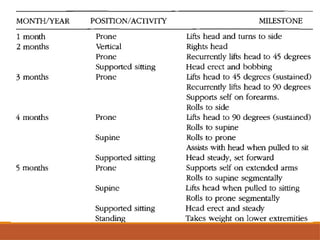
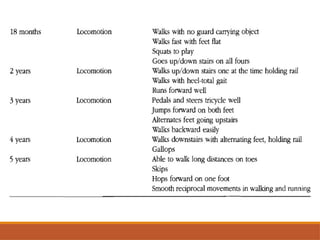
NEONATE-ONE MONTH
Momentary neckextension
Reflexive flexion posture
No functional muscle has developed
Hip are flexed with weight bearing on head and upper limb
Symmetrical in supine
Limbs retracted assuming position of abduction and flexion
Pronounced head lag, rounding of back, no extensor tone
No rotation except for neck righting, rooting reflex stimulates rotations
Hands fisted mostly, grasp reflex
Eye able to focus with in a limit range
15.
TWO MONTH
Prone:
Neck extensiondevelop to 45 degree
Extension developing down trunk
Tension in down trunk and upper limb appear
Still no scapular stabilization
Back less rounded in sitting due to extensor tone
developing
16.
TWO MONTH
Supine:
lack offlexor control
Pattern of flexion and extension with neck rotation appears
Rotation:
Lateral flexion and initial rotation influenced by galant and rooting
reflex
Hands:
Reflexive grasp, hands maintain flexed position
Involuntary release
Eyes:
Focusing improved
Coordination of hearing and vision
Follows moving object to midline, disassociation of head from
trunk
17.
THREE MONTH
Prone:
Neck extension
Chintucked
Increased extension in back and upper limb
Upper limb move forward and bear weight
Scapular stabilization
Less flexion at hips but no full weight bearing yet
18.
THREE MONTH
Flexion:
Increased flexioncontrol
Improved balance between flexors and extensor
Head has more midline orientation
Hands coming together to midline especial when
holding a toy
Eye focus in midline
Head in alignment with trunk
19.
THREE MONTH
Rotation:
Weight bearingon forearm
Head turning creates weight shift
Sensation of rotation beginning
If unable to shift weight, rotation may
not develop
20.
THREE MONTH
Hands:
Reaches outwith both upper limbs
Lunges at object and can make contact, may or
may not able to grasp
Brings hand together and looks at them
Might suck fingers or fists
Beginning to pull at clothing
Continue to scratch surface
Retains object using an ulnar grasp as opposed
to the palmar reflex grasp
21.
THREE MONTH
Eye:
Follow slowmoving object through 180
degree
May see head rotating with eyes
Reaches with eyes when held in sitting
position
22.
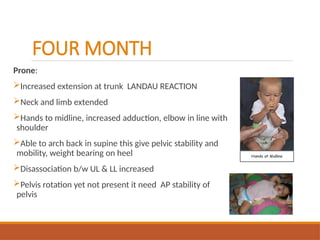
FOUR MONTH
Prone:
Increased extensionat trunk LANDAU REACTION
Neck and limb extended
Hands to midline, increased adduction, elbow in line with
shoulder
Able to arch back in supine this give pelvic stability and
mobility, weight bearing on heel
Disassociation b/w UL & LL increased
Pelvis rotation yet not present it need AP stability of
pelvis
23.
FOUR MONTH
Supine:
Increased flexorcontrol
Head in midline
LL continue to be abducted
Hands and upper limb more in midline
Scapular stability increased
Increased weight shift bilaterally
Gross grasp continuing on ulnar side
Eyes follow object smoothly
24.
FIVE MONTH
Extension:
Sitting lesssupport
Increased extension and scapular stability
Limbs reaching forward
Shifting weight on forearm
Reaching with hand open(ulnar release)
Less flexion on hip
Neck stable
Equilibrium reaction begin in prone
Foot to mouth causes elongation of lower spine and
neck.
25.
FIVE MONTH
FLEXION
Pull tosit with no head and neck lagging
Starts to lift and flex lower limbs
Abdominal control developing with pelvic stability
Weight shift side lying
Rotation in upper trunk
Stability and mobility in shoulder girdle
In side lying shoulder retract
Can roll back to supine,
Rolling prone to supine by neck extension and flexion, roll like a log
Grasps object in front of face
Use palmar grasp with increased use of radial digit
Can lift a cube, slap, pat, raking movements with fingers
Bilateral hand approach due to ulnar and radial release
Maintain fixation on self
26.
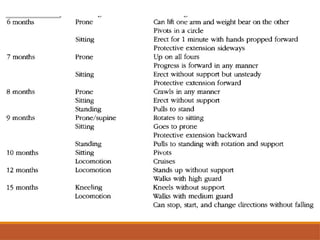
SIX MONTH
Sit withback straight
Strong landau
Balance tone in flexors and extensor
Stands weight bearing positive supporting
Pull to sit: active flexion of neck, abdominal
control with raise lower limb
Good balance between flexion and extension
Righting reaction starts
Equilibrium reaction in supine
Weight shift to extended upper limb, more
control in shoulder and scapulae
27.
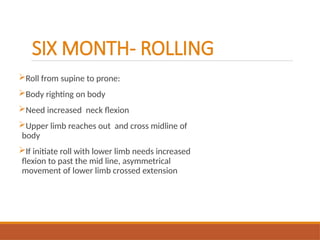
SIX MONTH- ROLLING
Rollfrom supine to prone:
Body righting on body
Need increased neck flexion
Upper limb reaches out and cross midline of
body
If initiate roll with lower limb needs increased
flexion to past the mid line, asymmetrical
movement of lower limb crossed extension
28.
SIX MONTH-HANDS
Radial palmargrasp
If drops object may rescue it
Transfer objects from hand to other
Reaches out with one hand while holding object other
Pats image in mirror
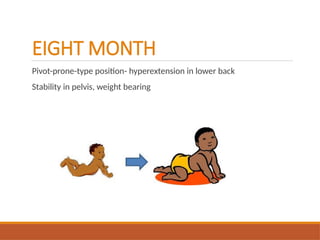
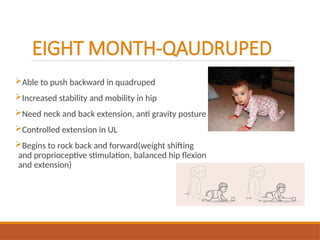
EIGHT MONTH-QAUDRUPED
Able topush backward in quadruped
Increased stability and mobility in hip
Need neck and back extension, anti gravity posture
Controlled extension in UL
Begins to rock back and forward(weight shifting
and proprioceptive stimulation, balanced hip flexion
and extension)
31.
EIGHT MONTH- sitting
Sitwith balance
Able to push back into sitting, first symmetrically,
then develops asymmetrically side sitting position
using pelvis rotation and stability in shoulder
In sitting lower extremities have more extension to
recover balance
All component of extension are available
Able to pull stand with minimal abduction for
standing
32.
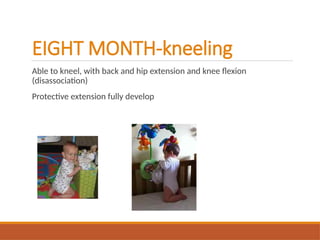
EIGHT MONTH-kneeling
Able tokneel, with back and hip extension and knee flexion
(disassociation)
Protective extension fully develop
33.
EIGHT MONTH-rotation
Pushes backinto quadruped position, rotates pelvis into side sitting
Begins lower extremities out in front for long sit position
Righting reaction, equilibrium reaction and disassociation of body parts
are in voluntary control
34.
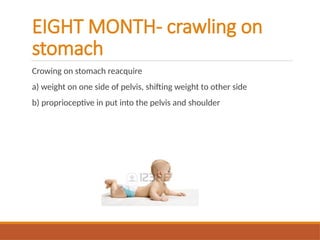
EIGHT MONTH- crawlingon
stomach
Crowing on stomach reacquire
a) weight on one side of pelvis, shifting weight to other side
b) proprioceptive in put into the pelvis and shoulder
35.
EIGHT MONTH- creeping
forward
Hassufficient trunk, shoulder, and pelvic girdle stability
Reciprocal movements
Half kneels using rotation
EIGHT MONTH- hands
Pincergrip
Increased maturity of neutral to supination but not complete
Crude voluntary release of objects
Fore finger isolation, beginning to isolate fingers
Pick up small objects with pincer grip
More advance use of hands combine with wrist extension and
supination
38.
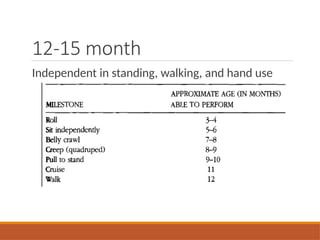
TEN MONTH
Independence insitting
Grasp and release function
Pincer position (finger and thumb) is available
voluntary
Can twist, turn, pivot and regain sitting balance
may be able to Bear walks on the hand
Control cruising sideways
Walks both hand held, LL in abd &ext rot
Initial standing (high guard upper extremities, abd &
ext rotation lower extremities)