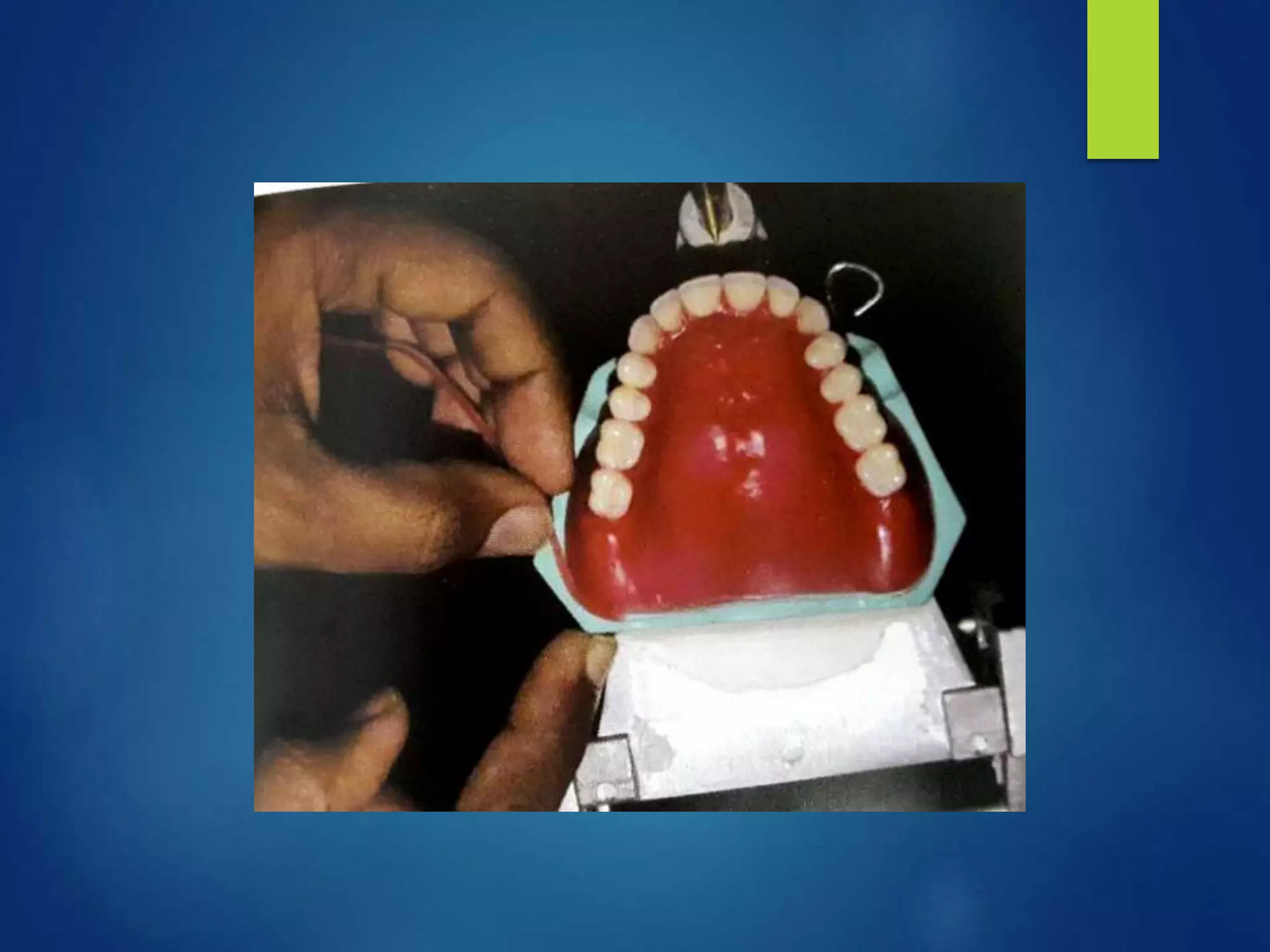
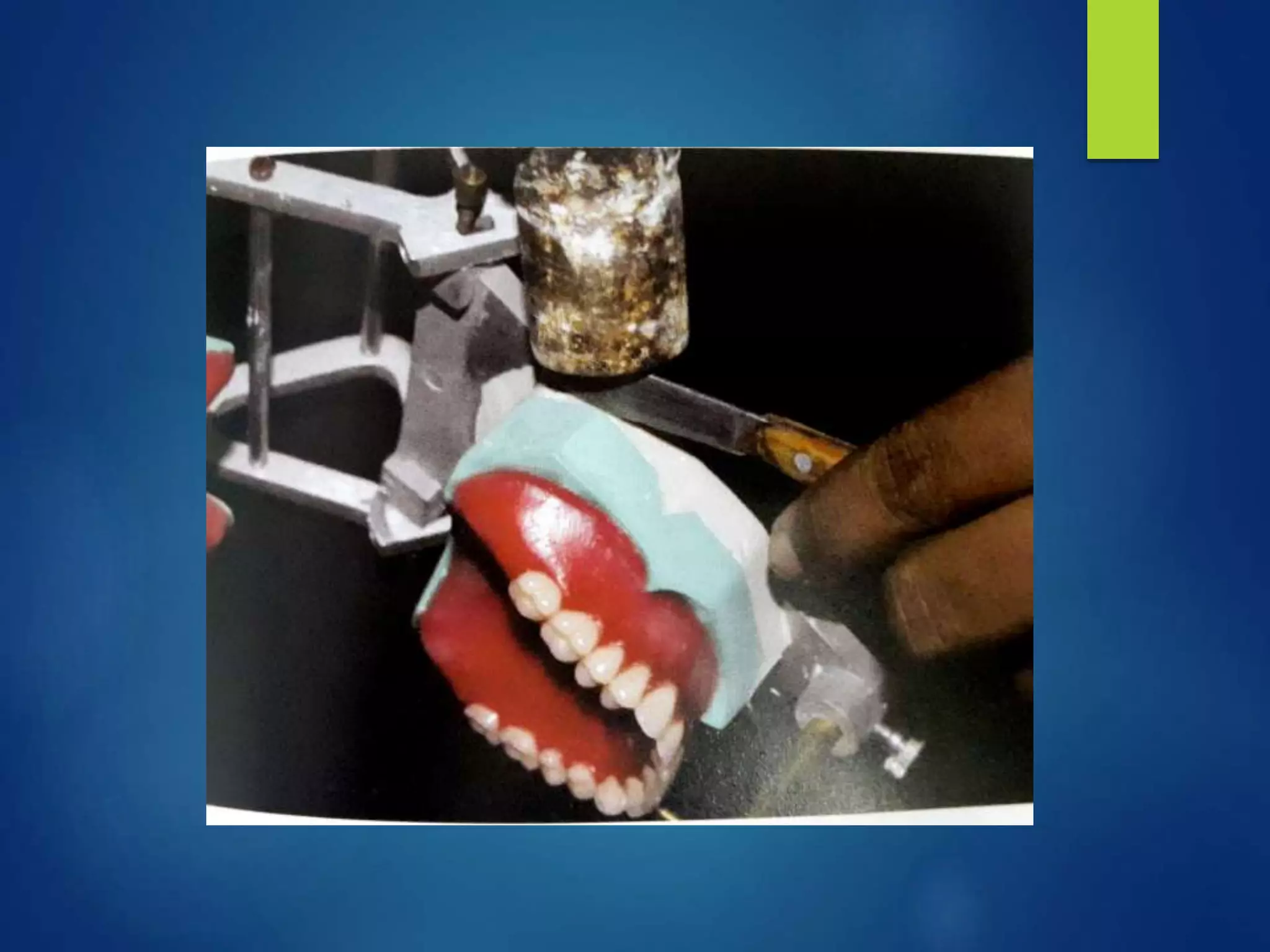
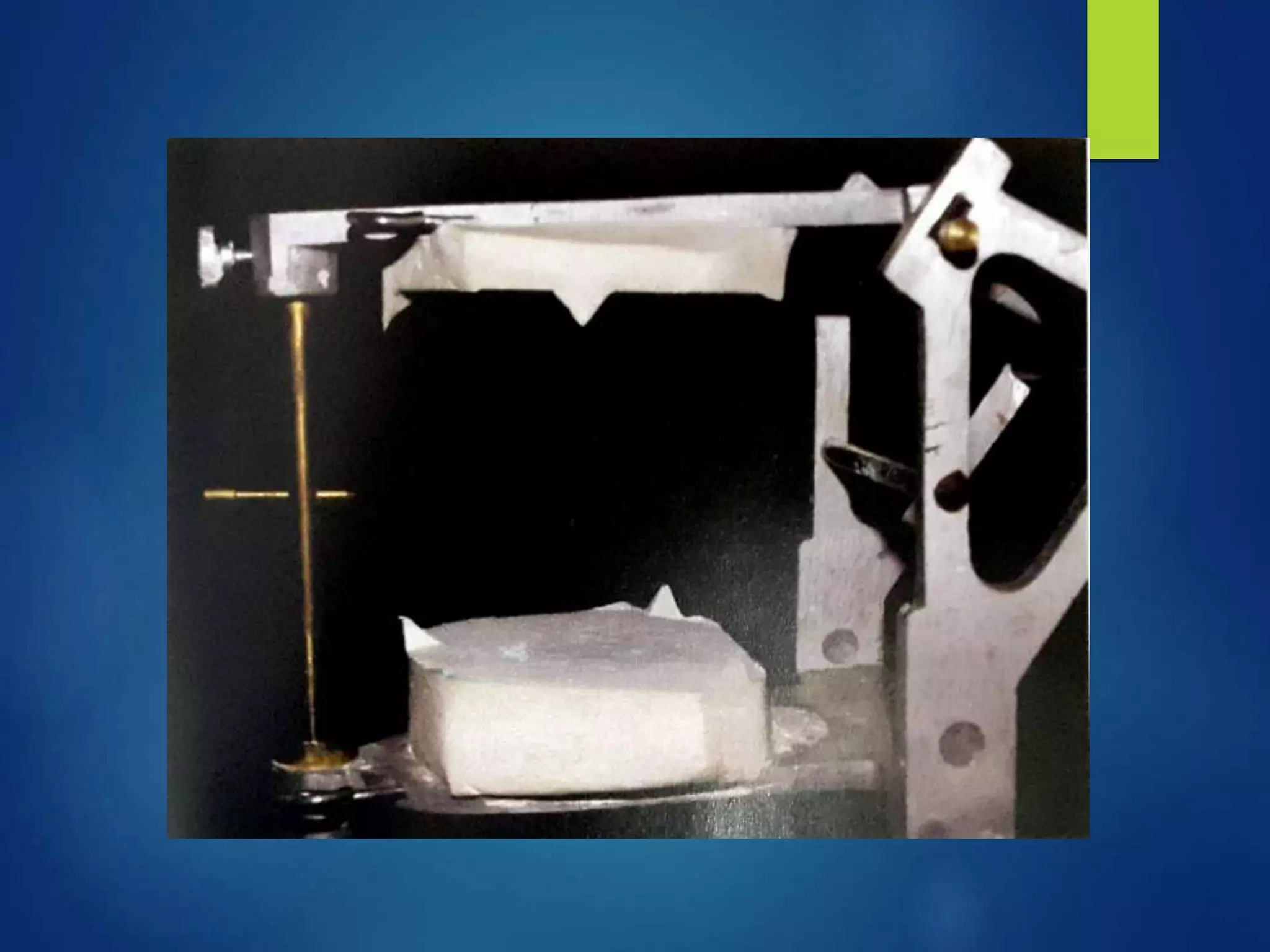
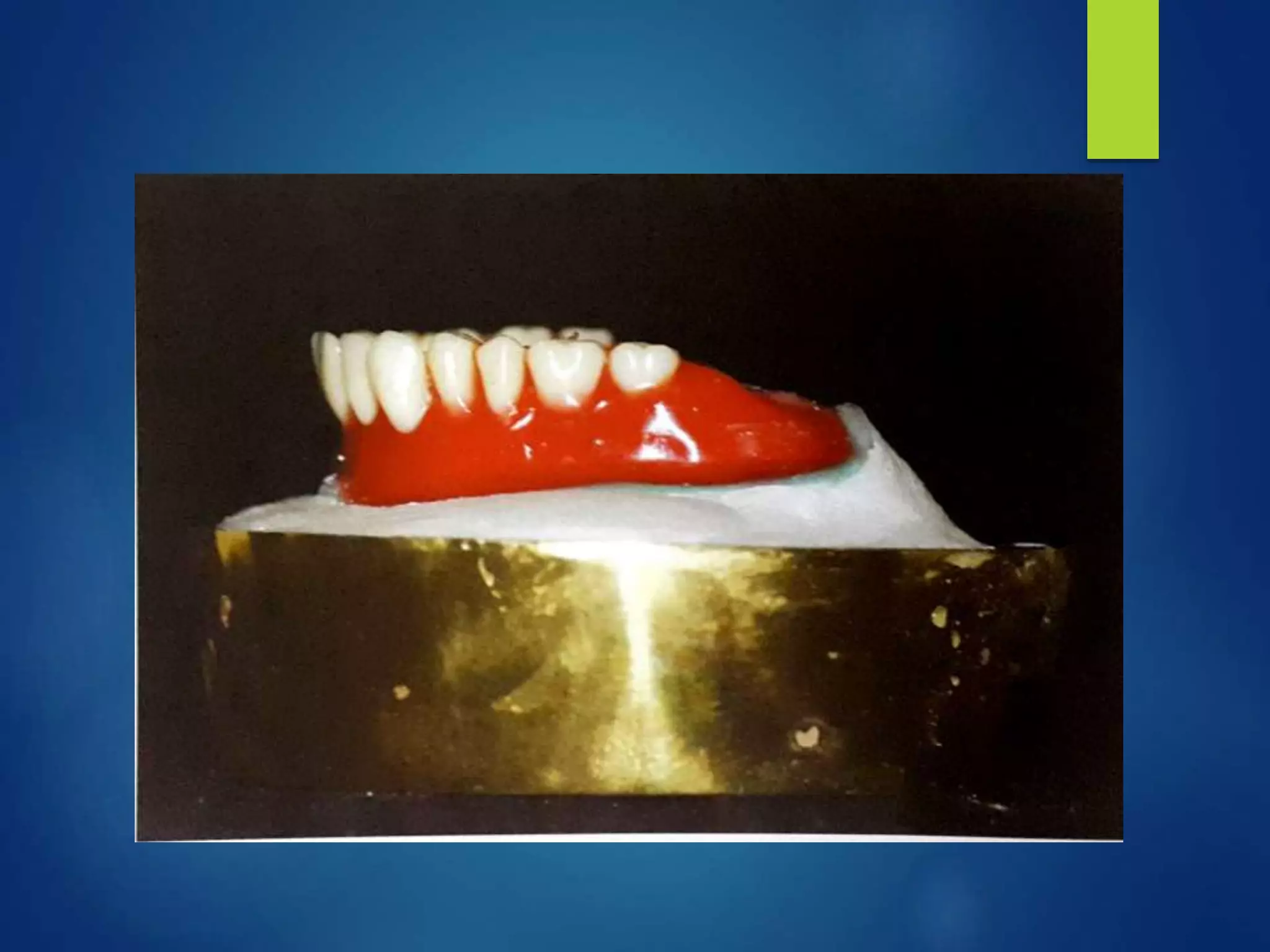
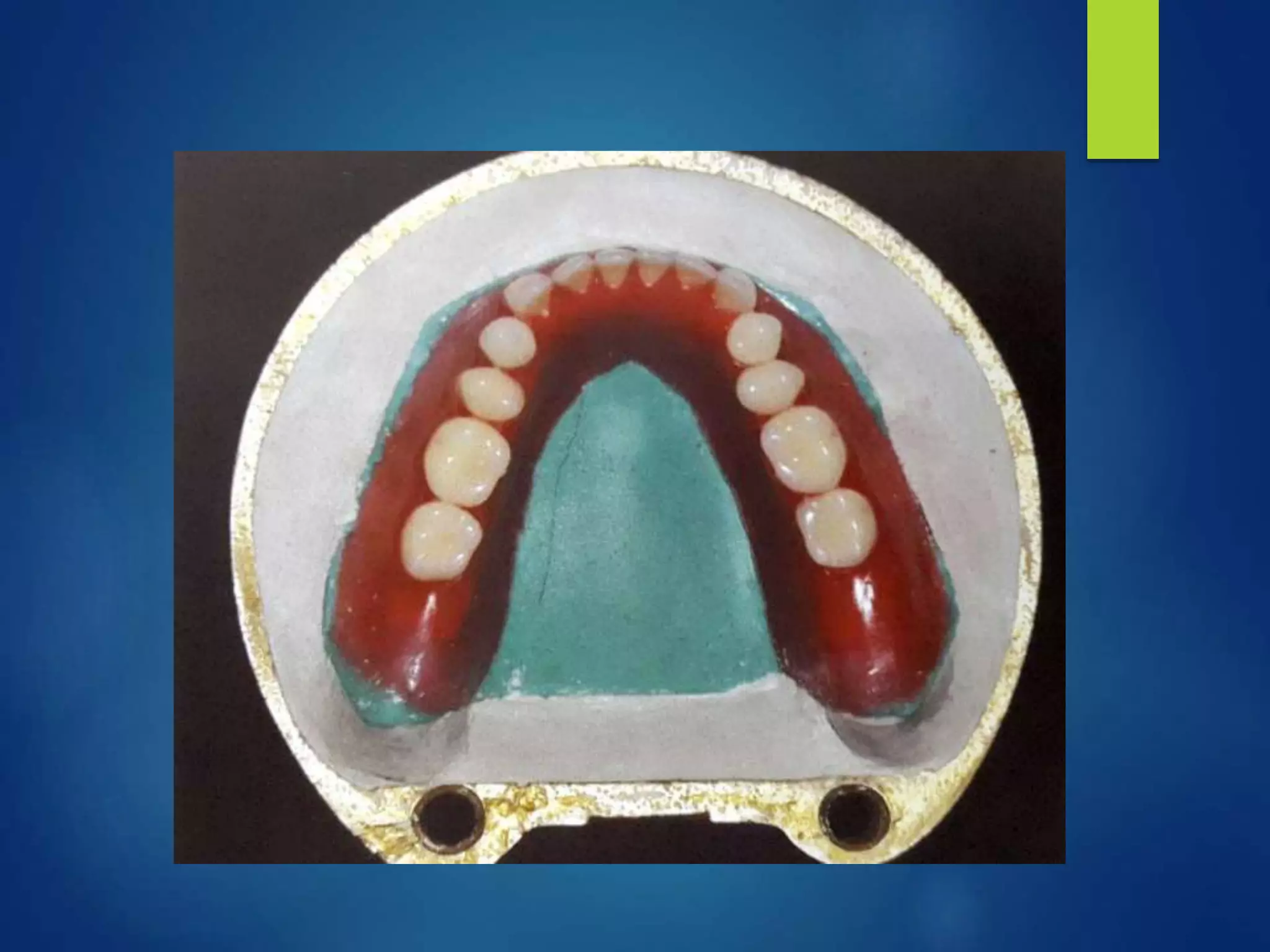
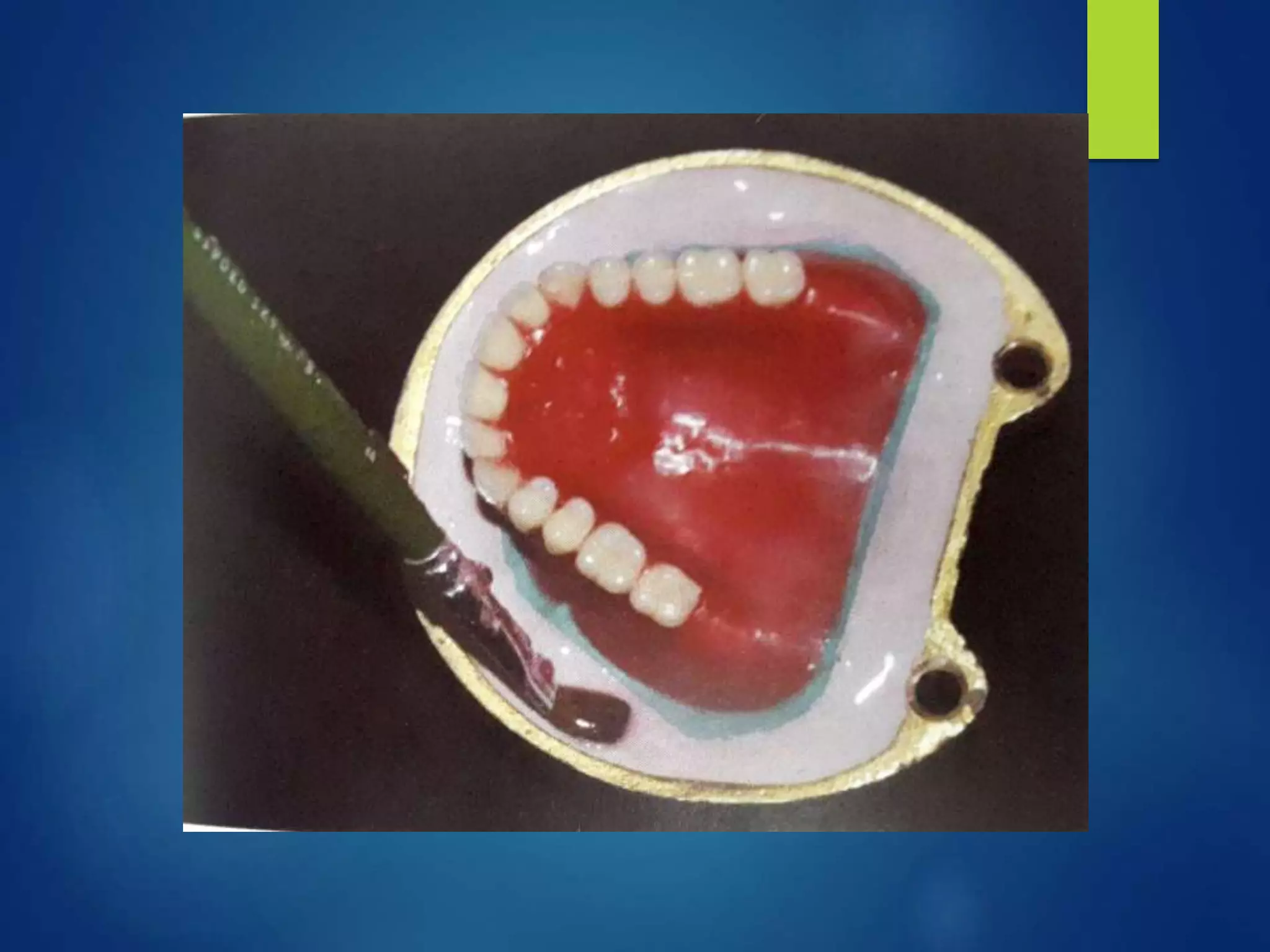
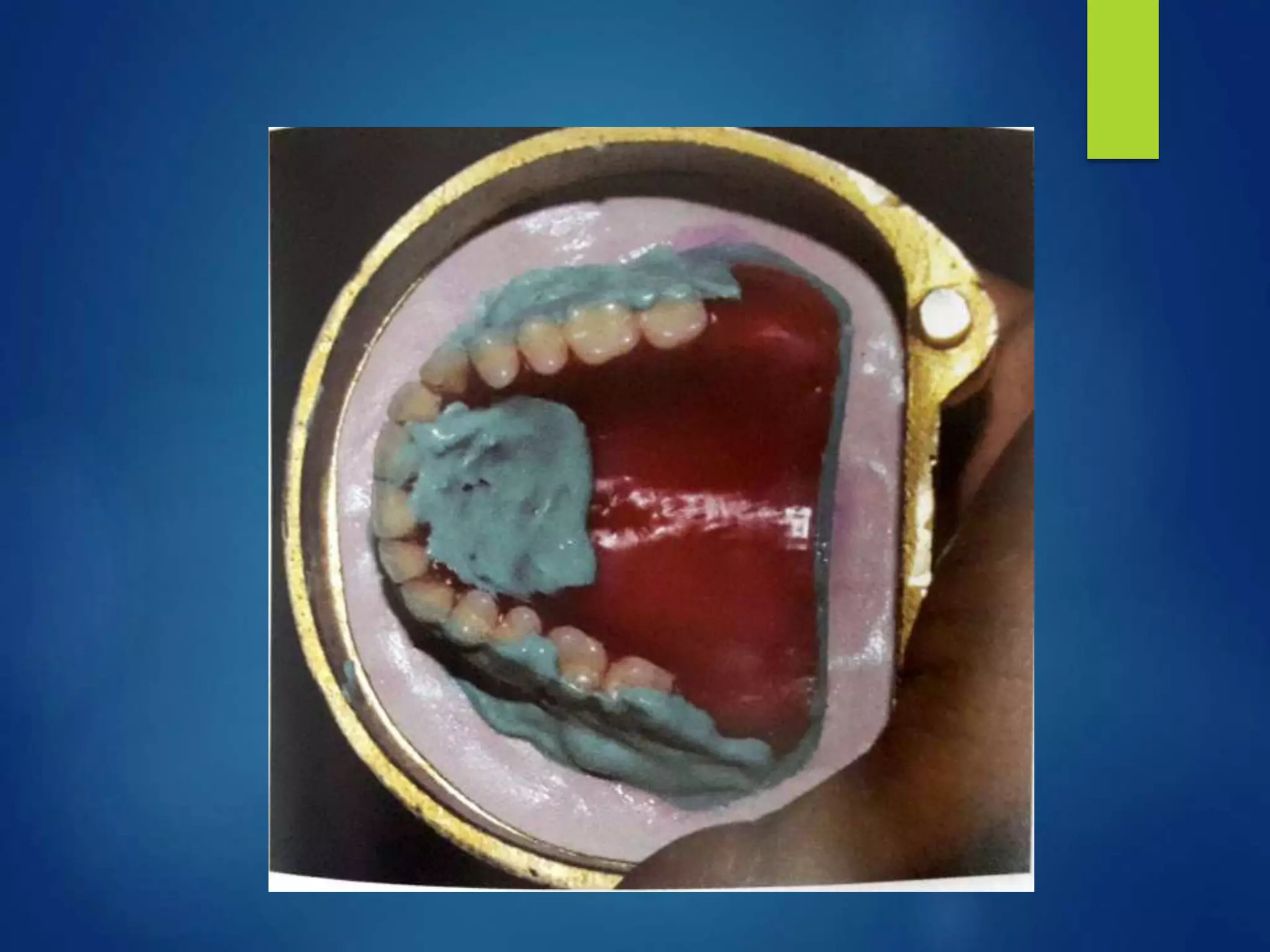
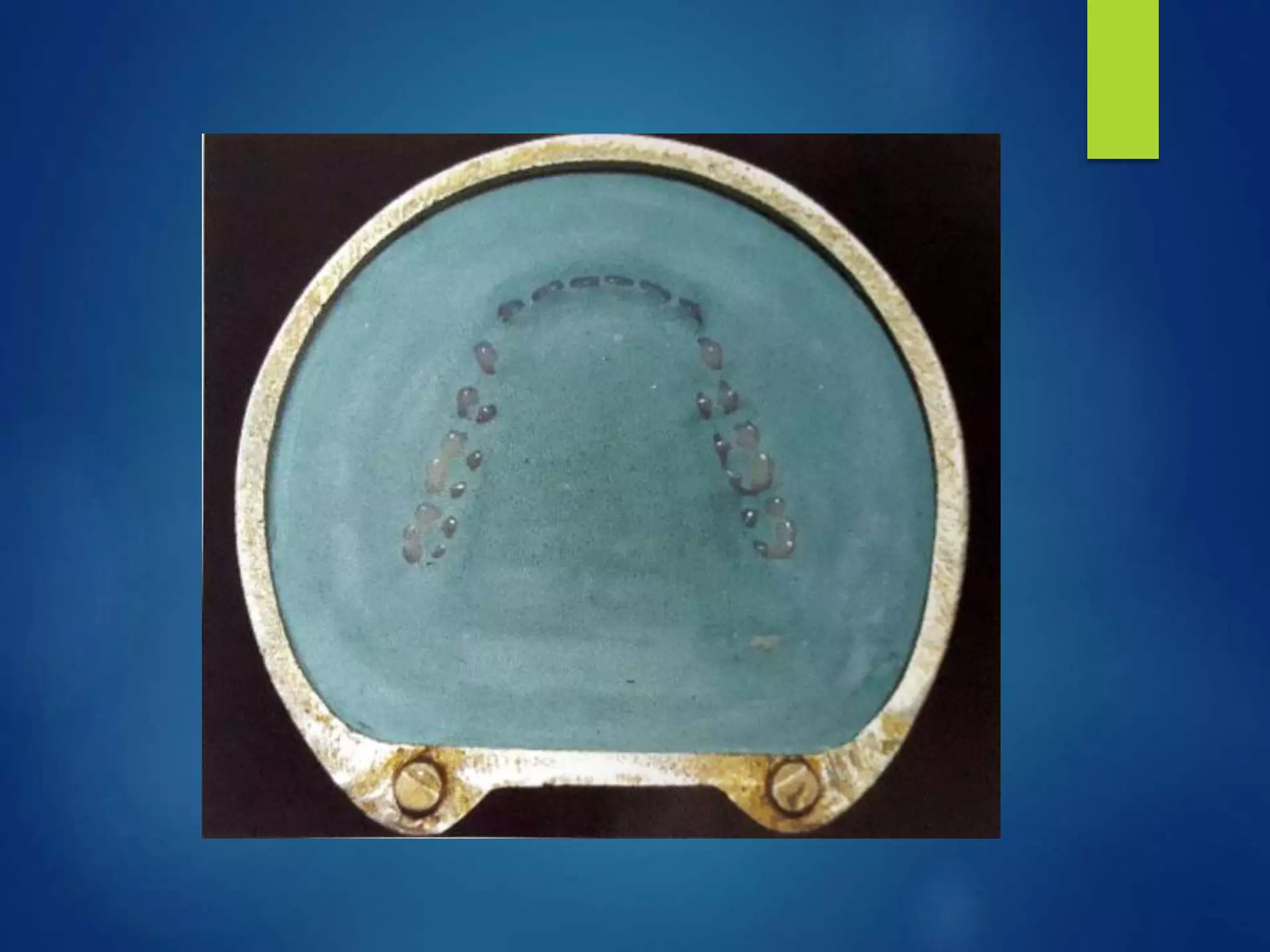
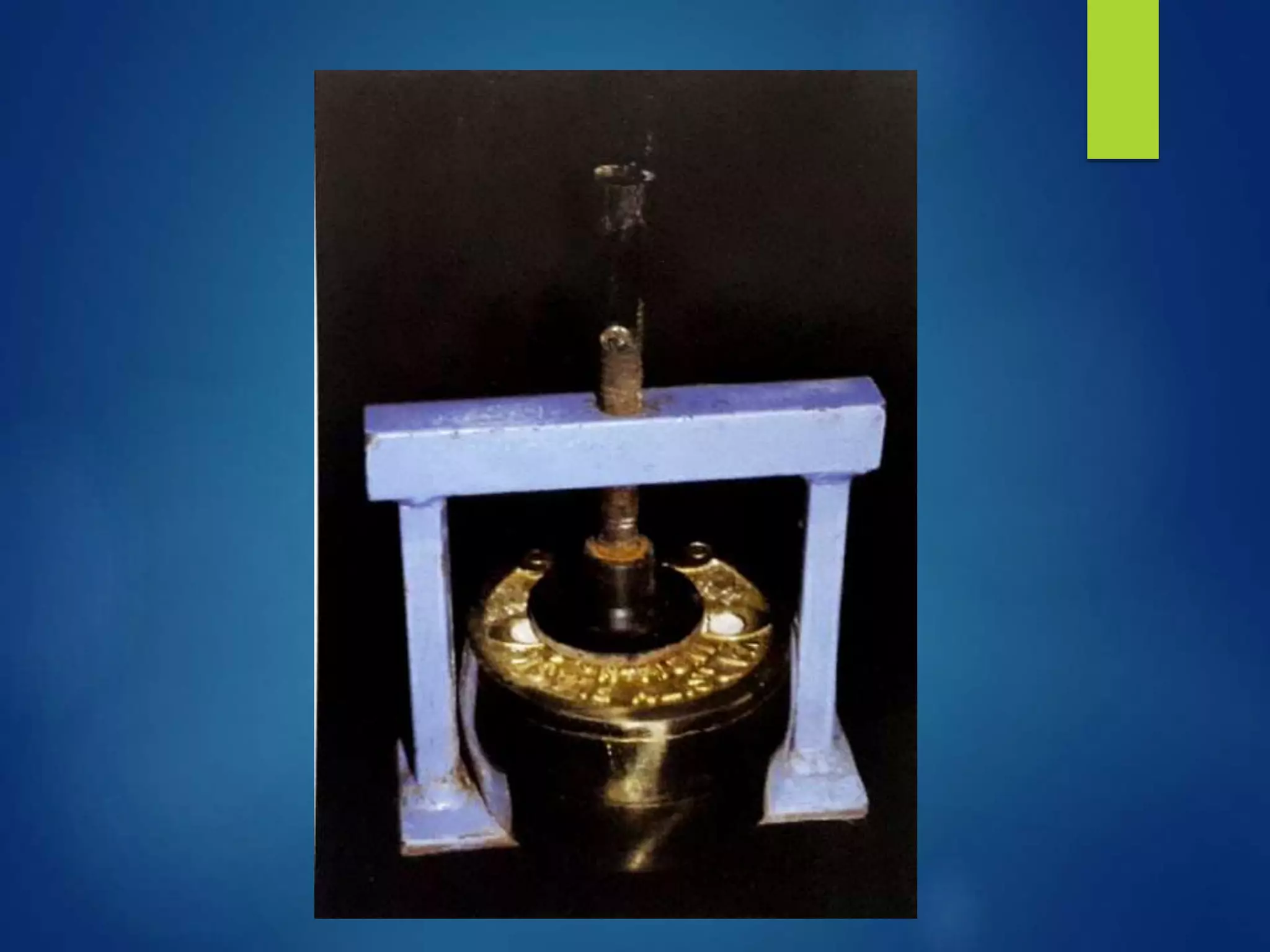
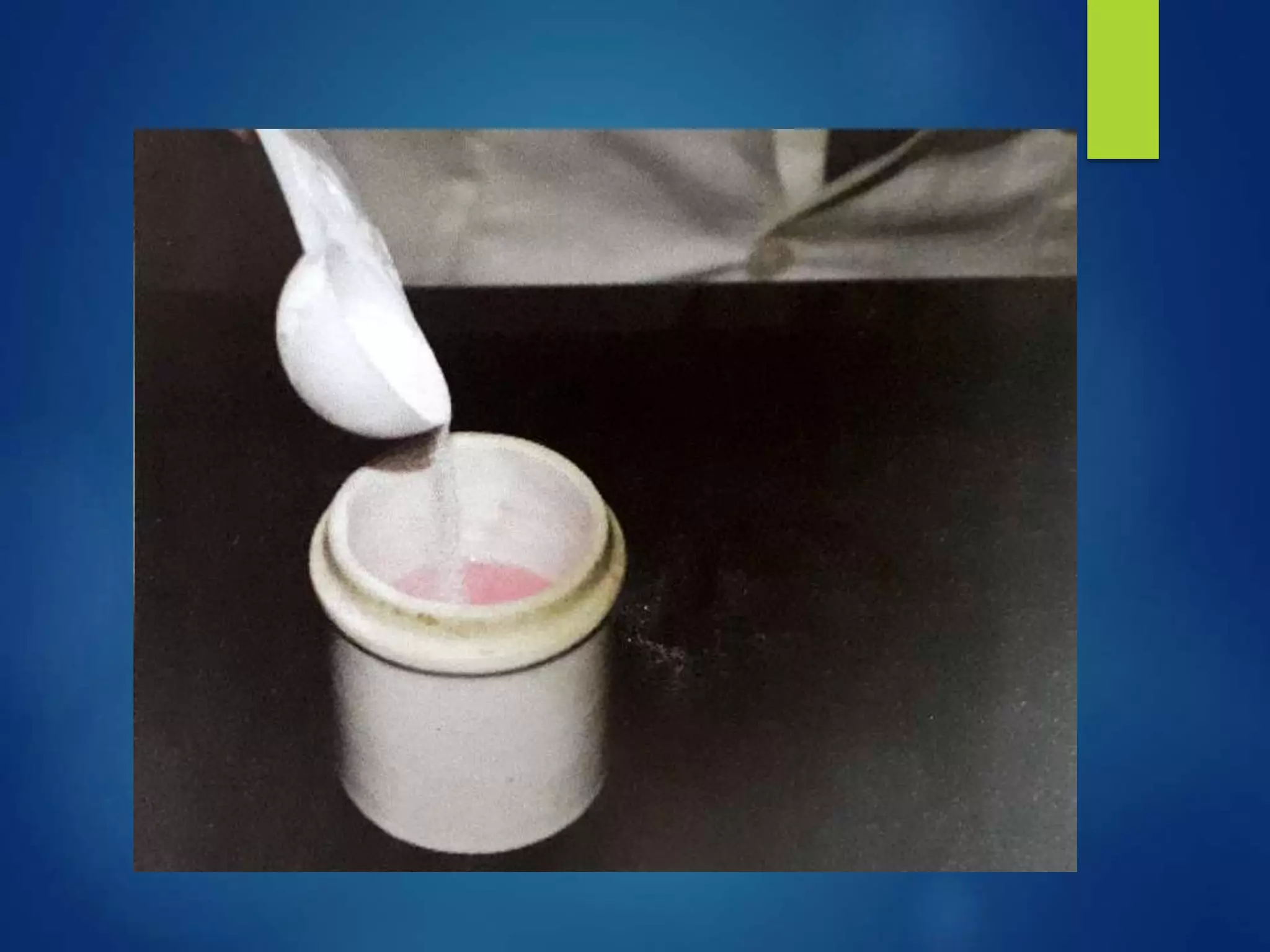
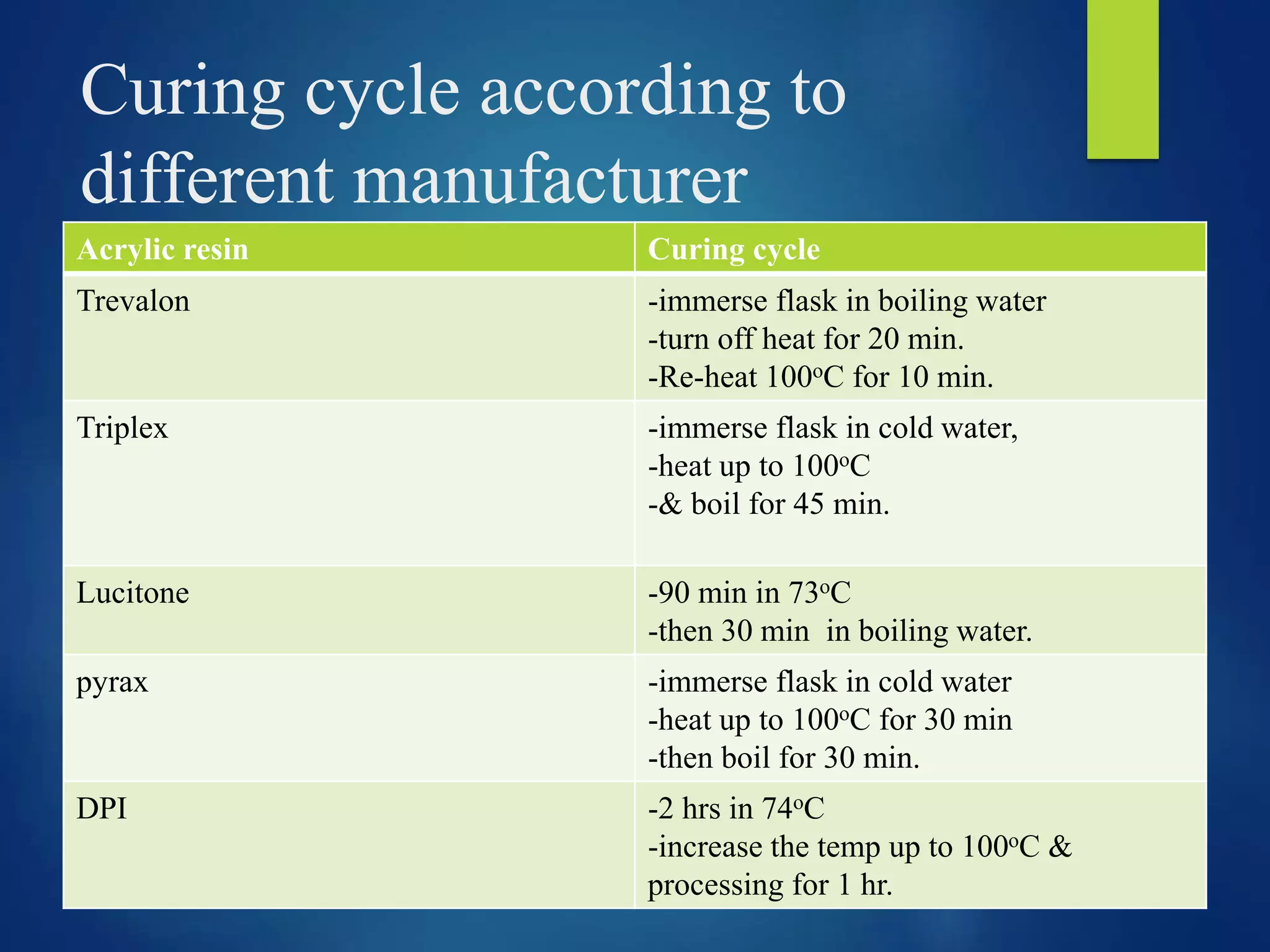
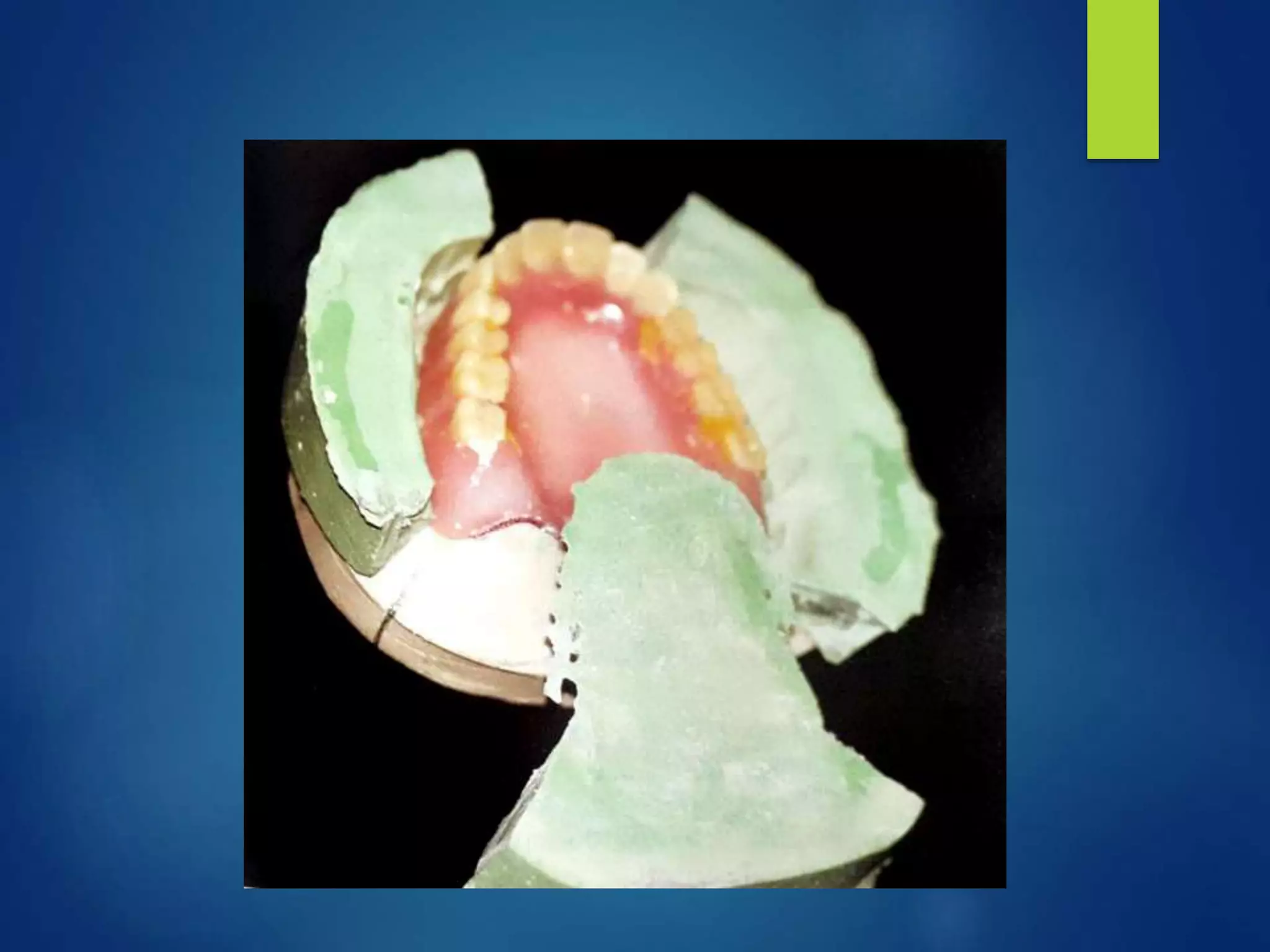
The document provides details on lab procedures for processing complete dentures after the try-in stage. It discusses acrylic resins used for denture bases, processing techniques including flasking, dewaxing, applying separating medium, mixing, packing, curing, and deflasking. Compression molding is the most common technique, involving preparing the trial denture, flasking, applying separating medium, mixing and packing the acrylic resin, curing using either a short or long cycle in a water bath, and finishing. The quality of processing is critical for the success of the final denture.