Download to read offline
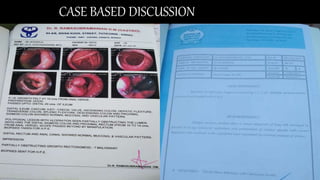





- The patient is a 36-year-old man who underwent neoadjuvant chemoradiotherapy in 2015 for rectal cancer. - In 2021, he presented with frequent urination. Imaging showed a large recurrent mass involving abdominal structures. - Biopsy of the skin deposit was suspicious for metastatic mucinous carcinoma. - The case discusses the current treatment approaches for locally advanced rectal cancer, including neoadjuvant and total neoadjuvant therapy options, and choices for chemotherapy and radiotherapy.























































































