Downloaded 753 times
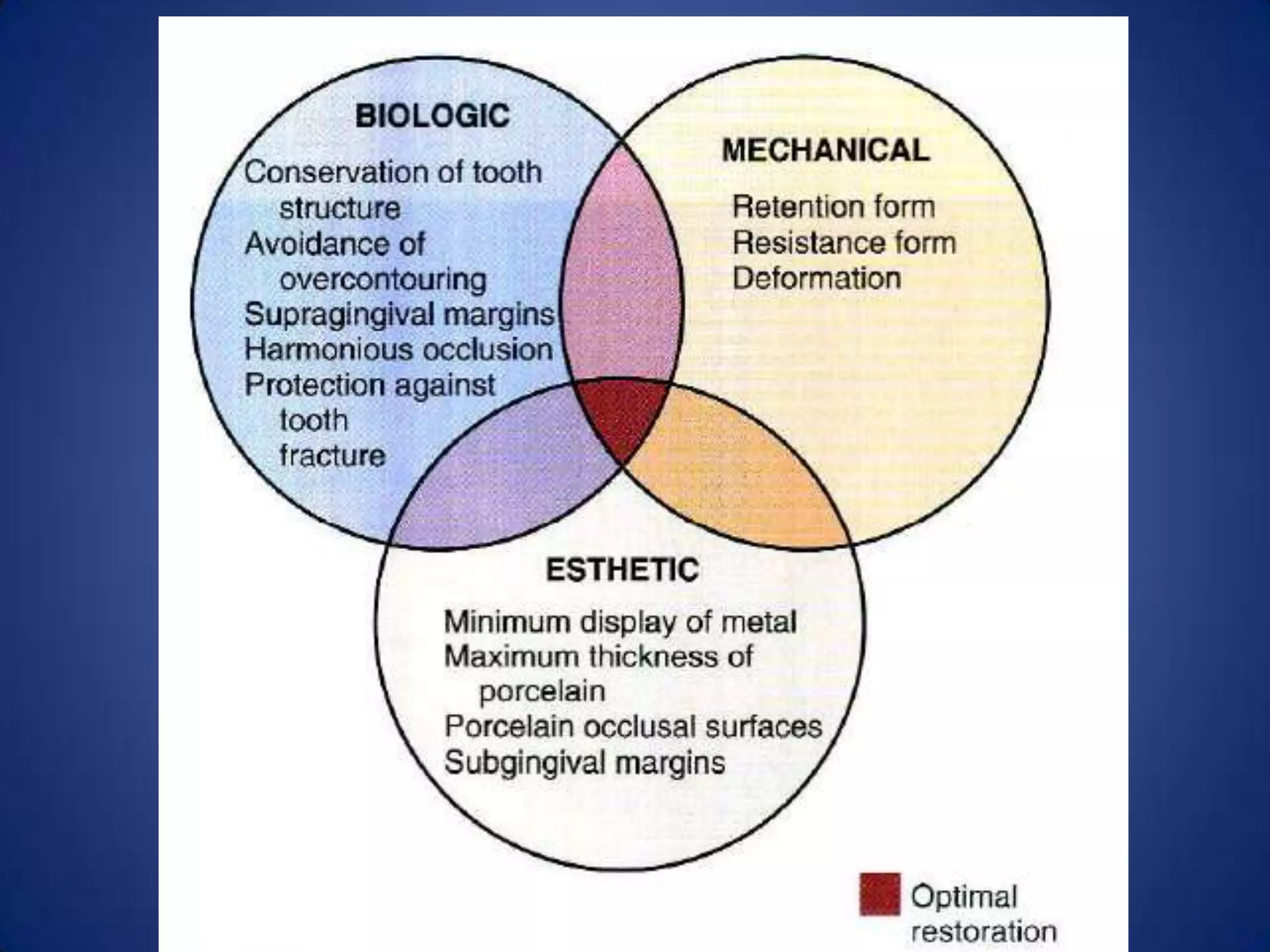

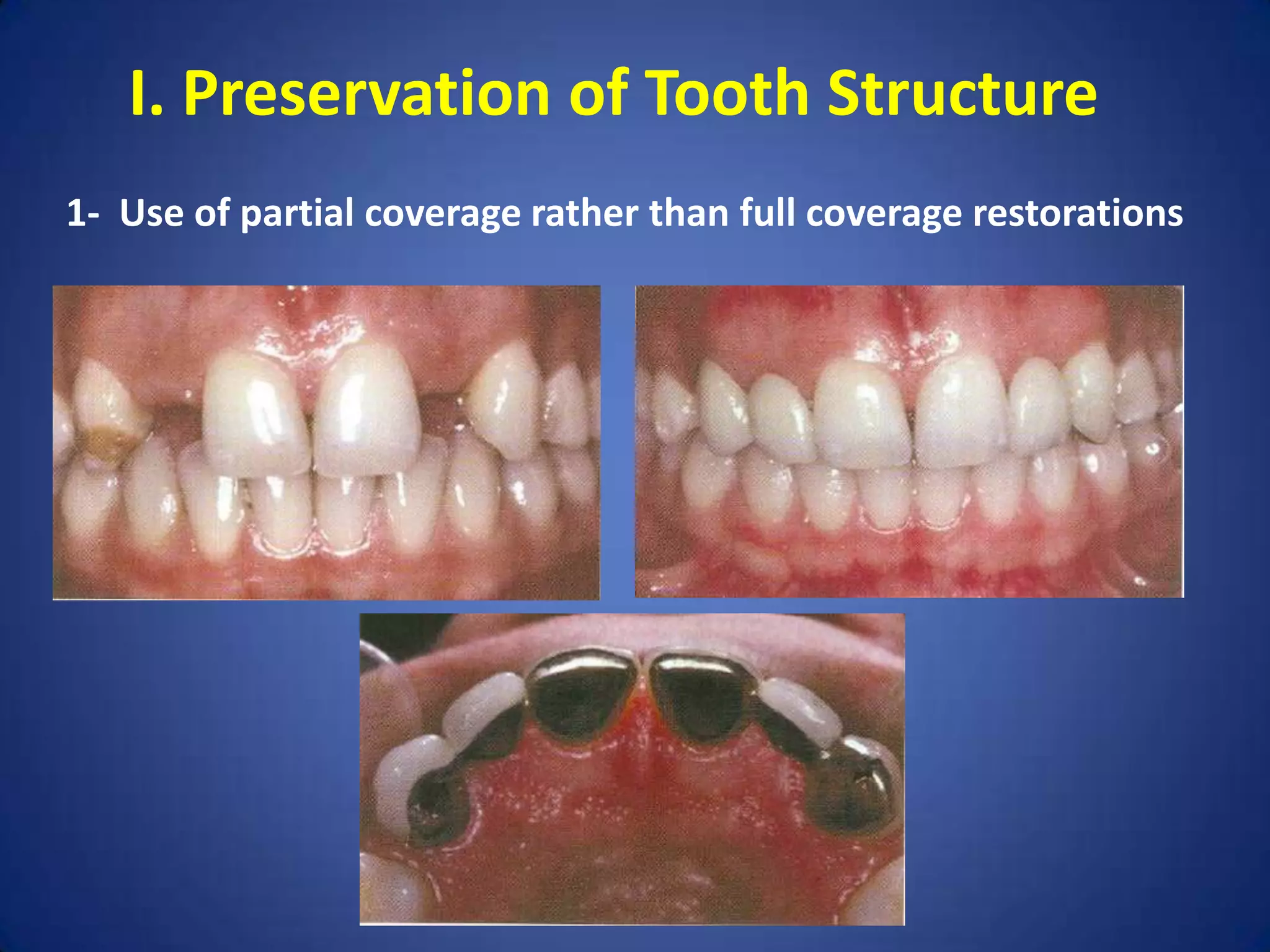
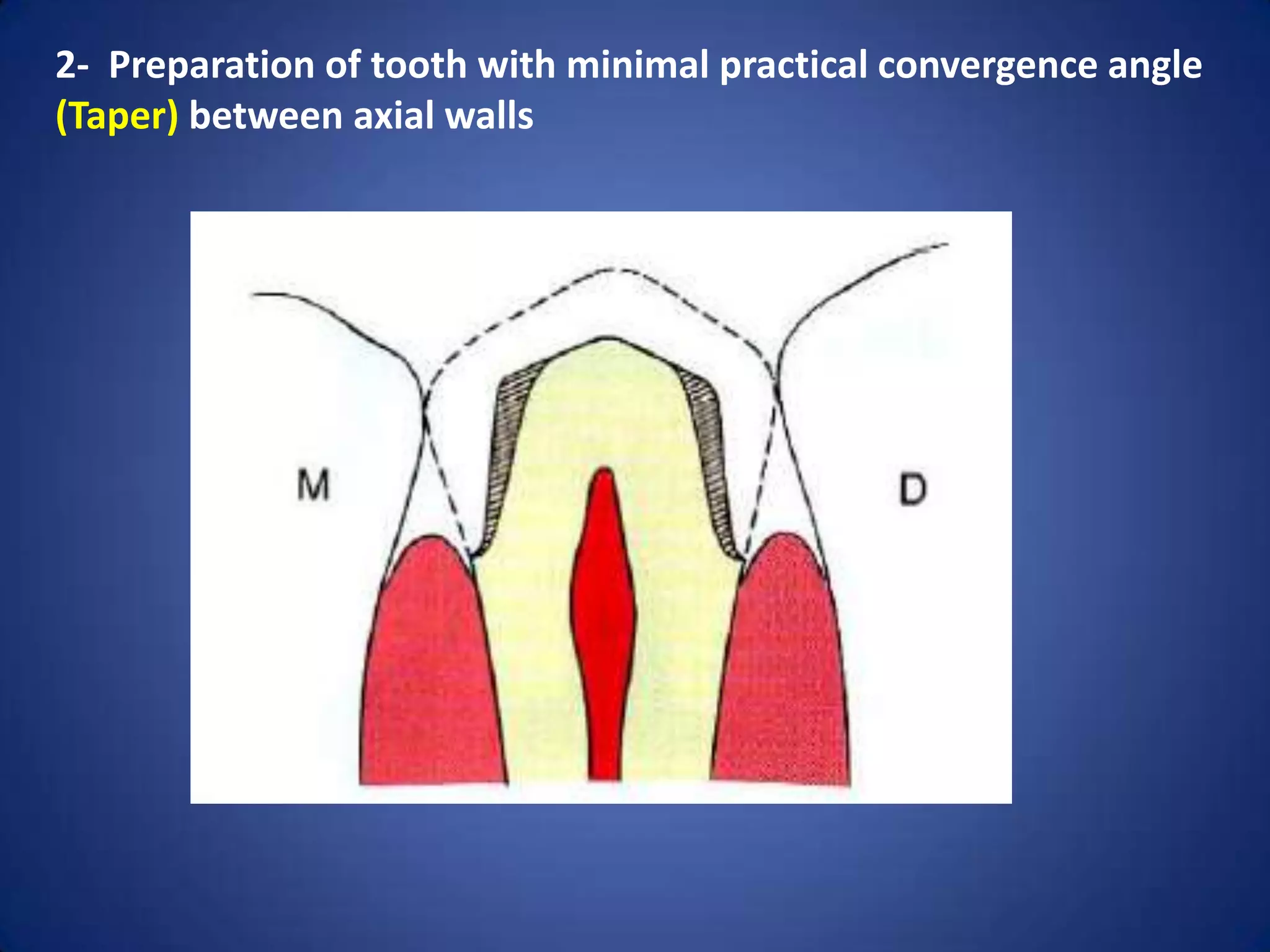
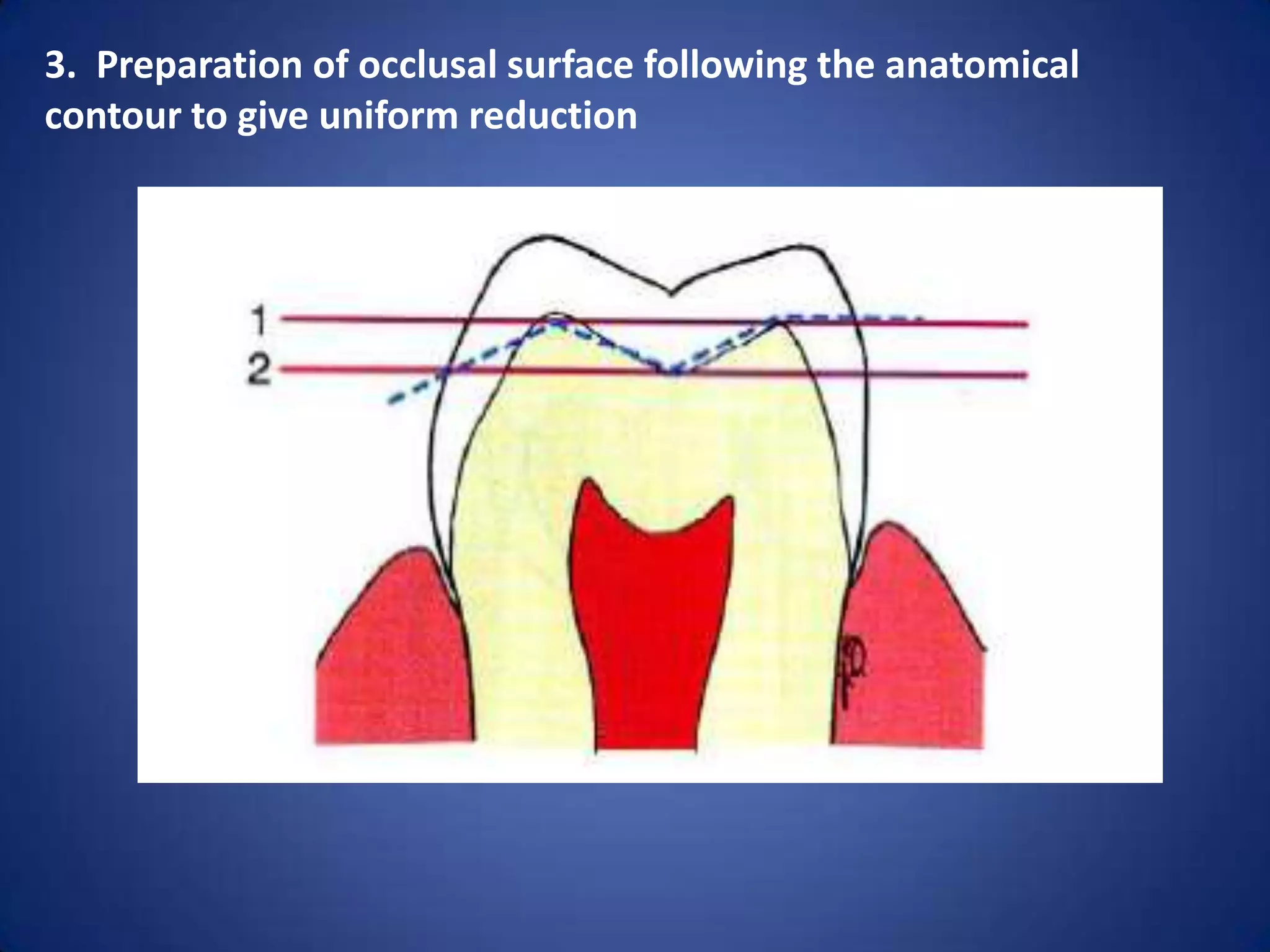
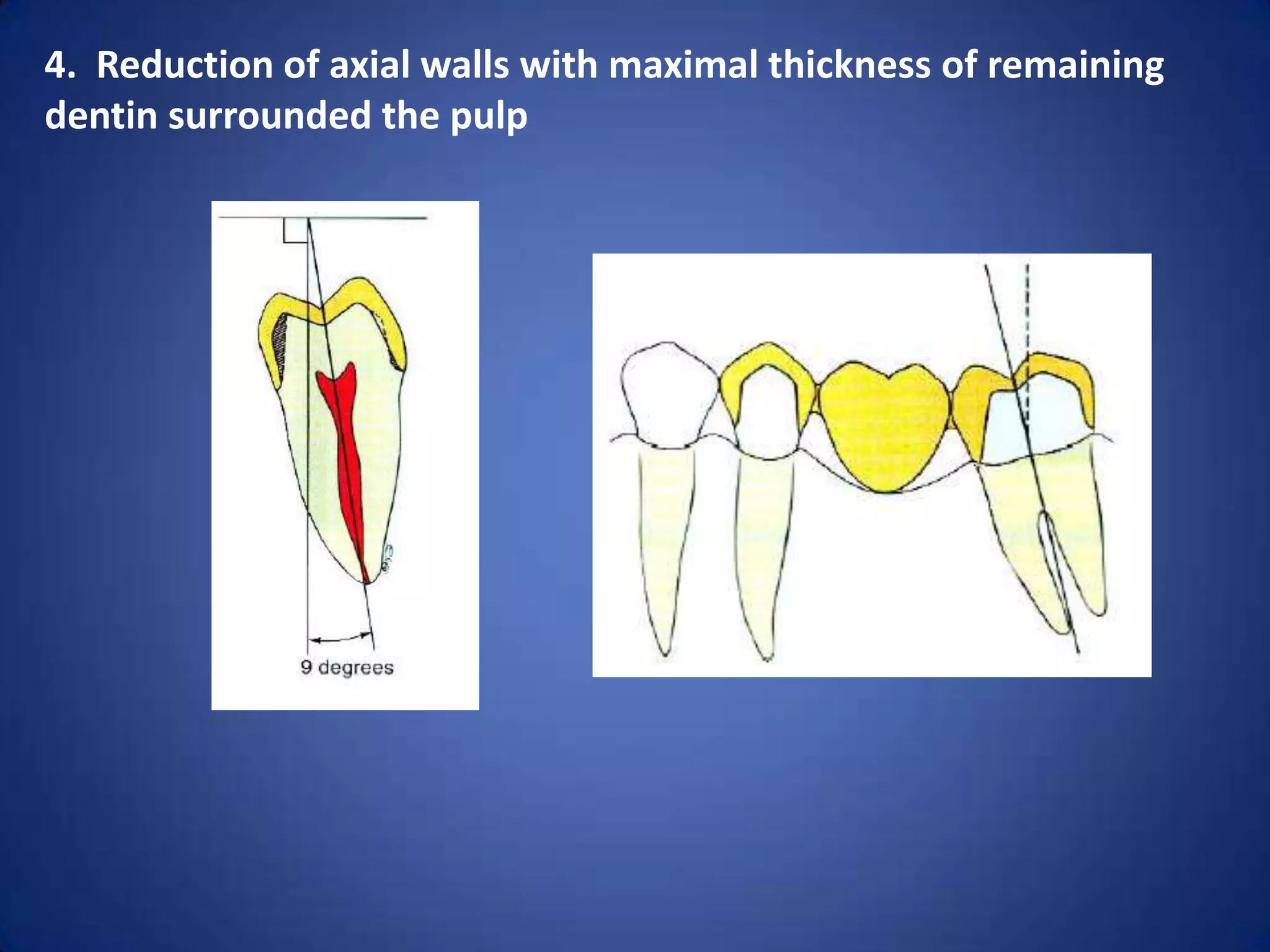
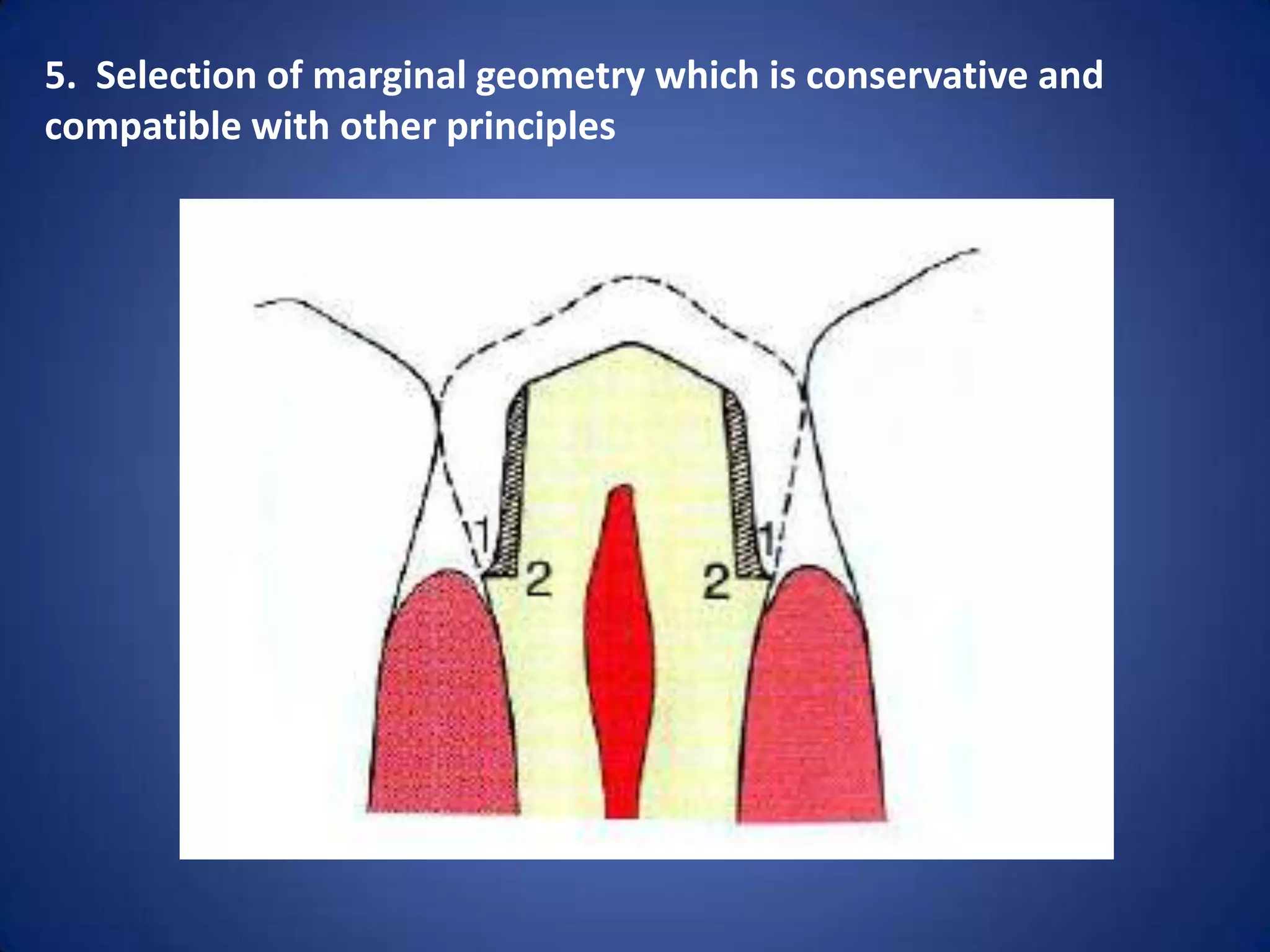
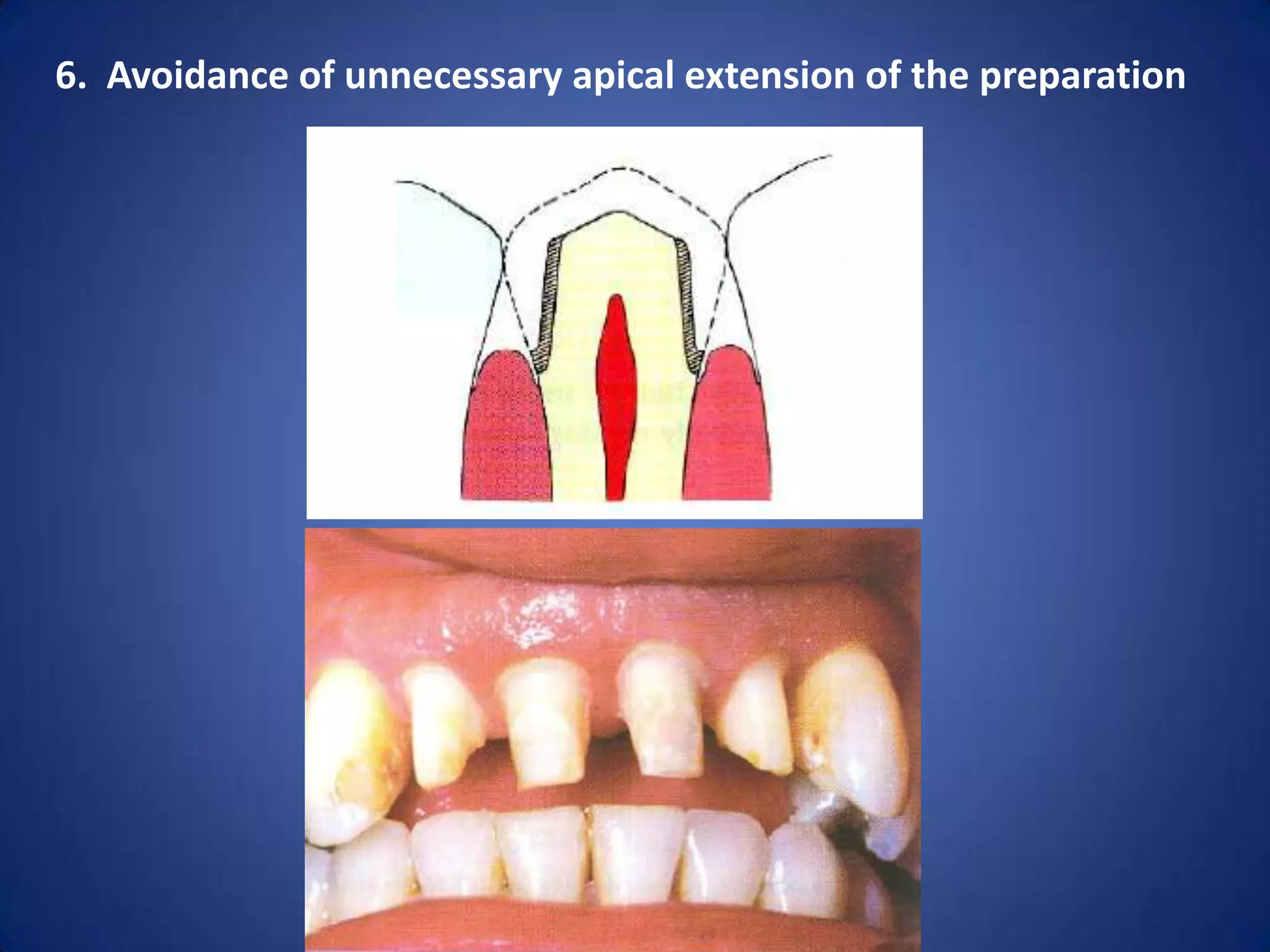
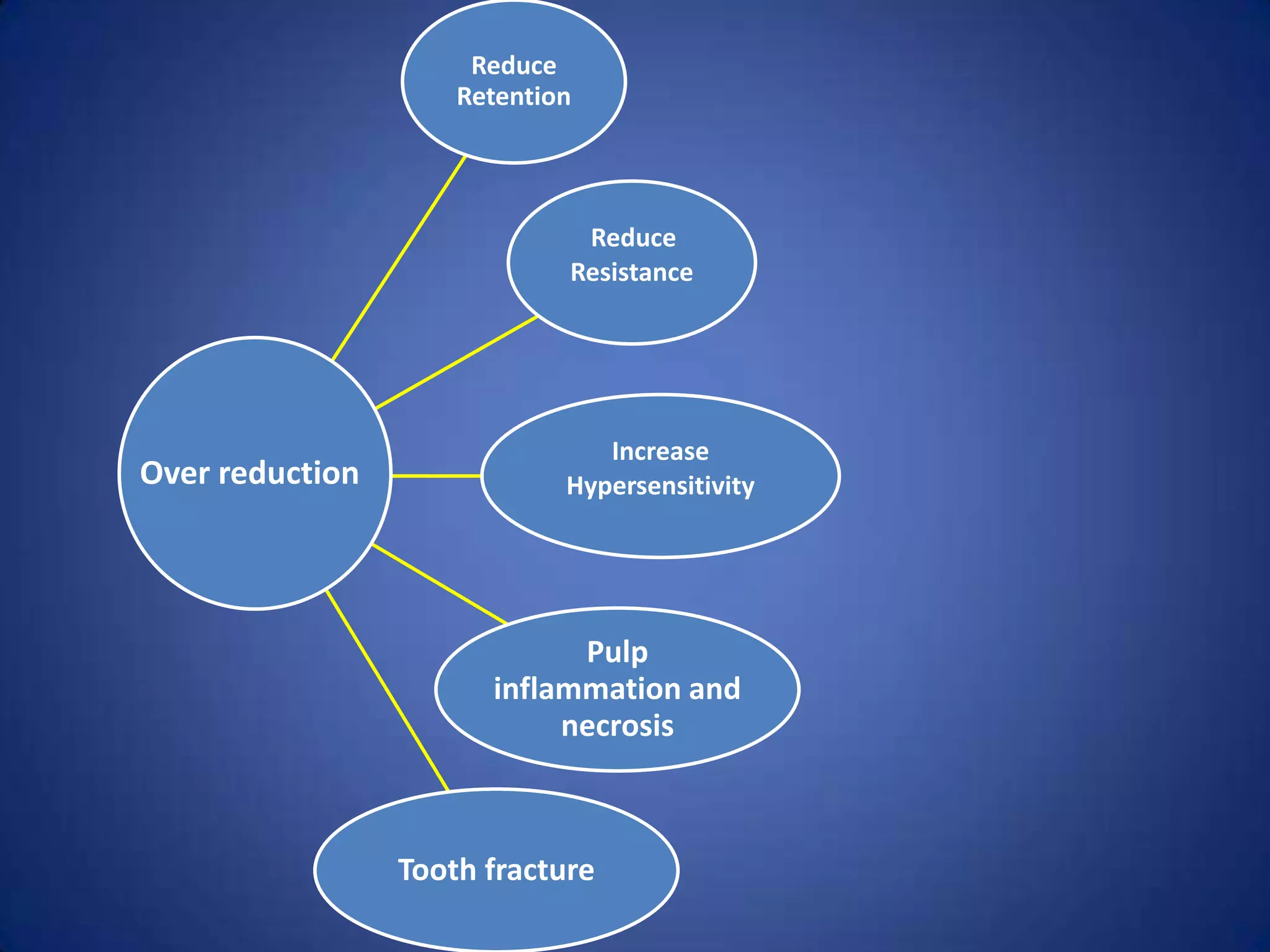
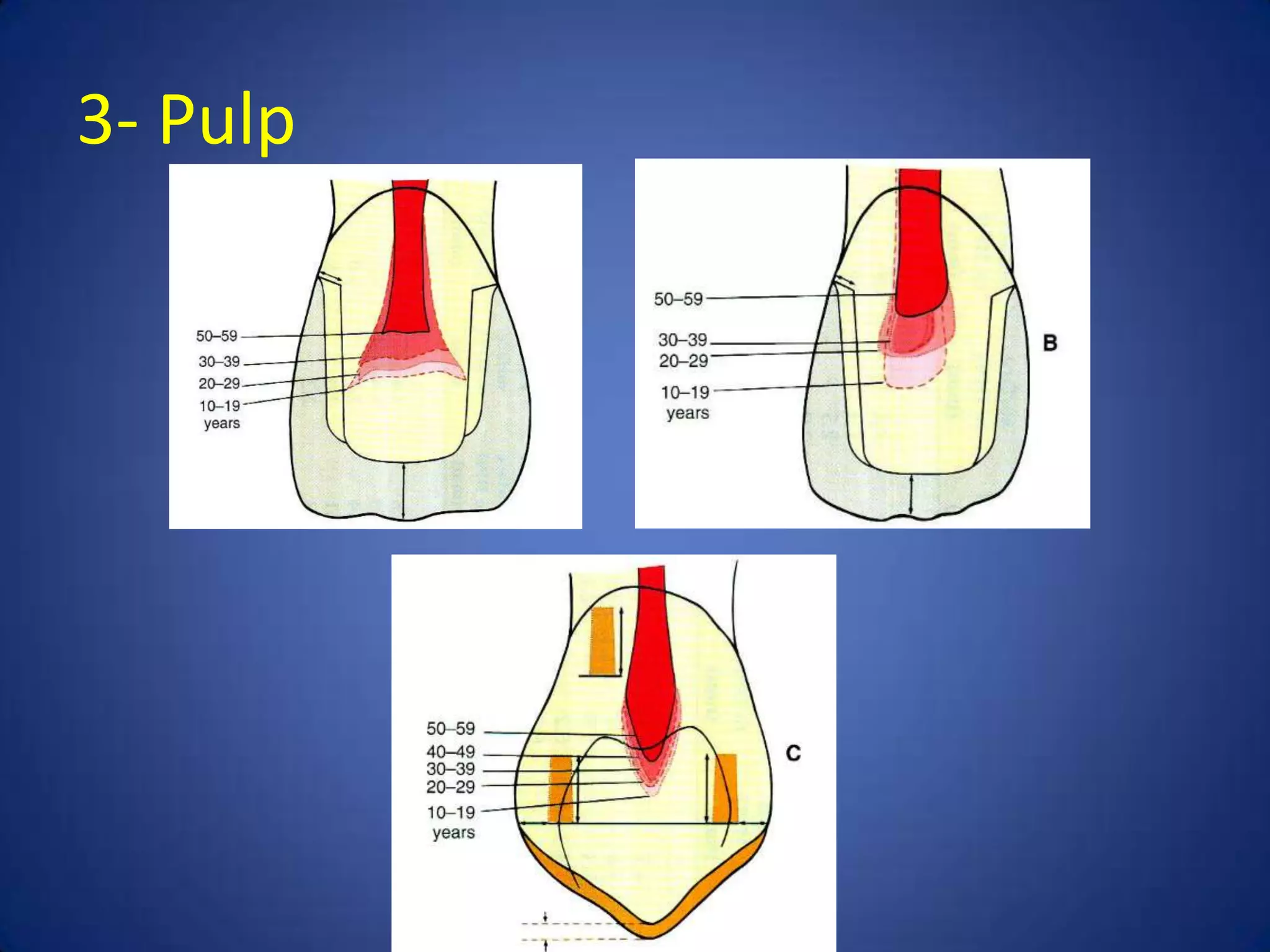
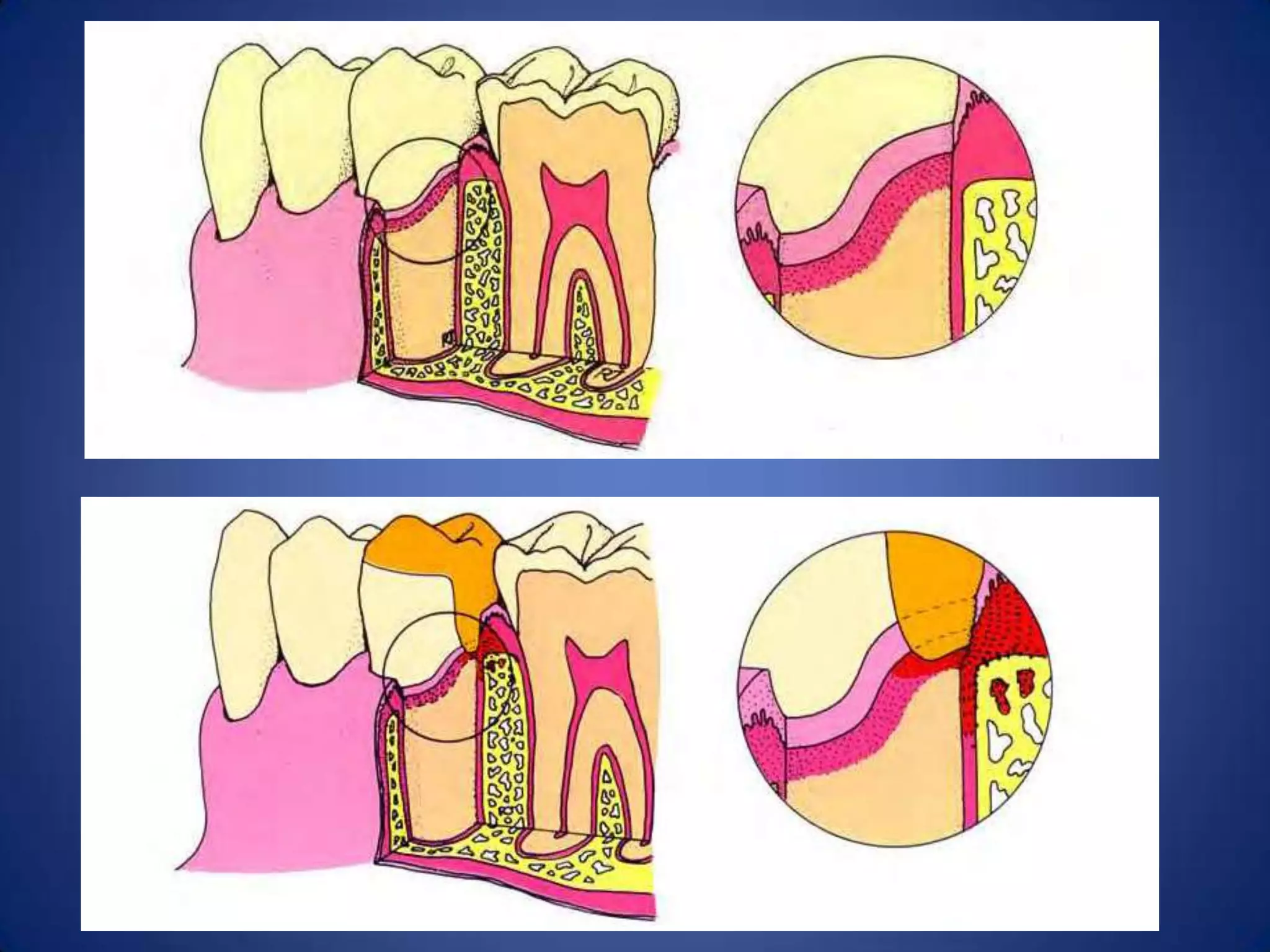

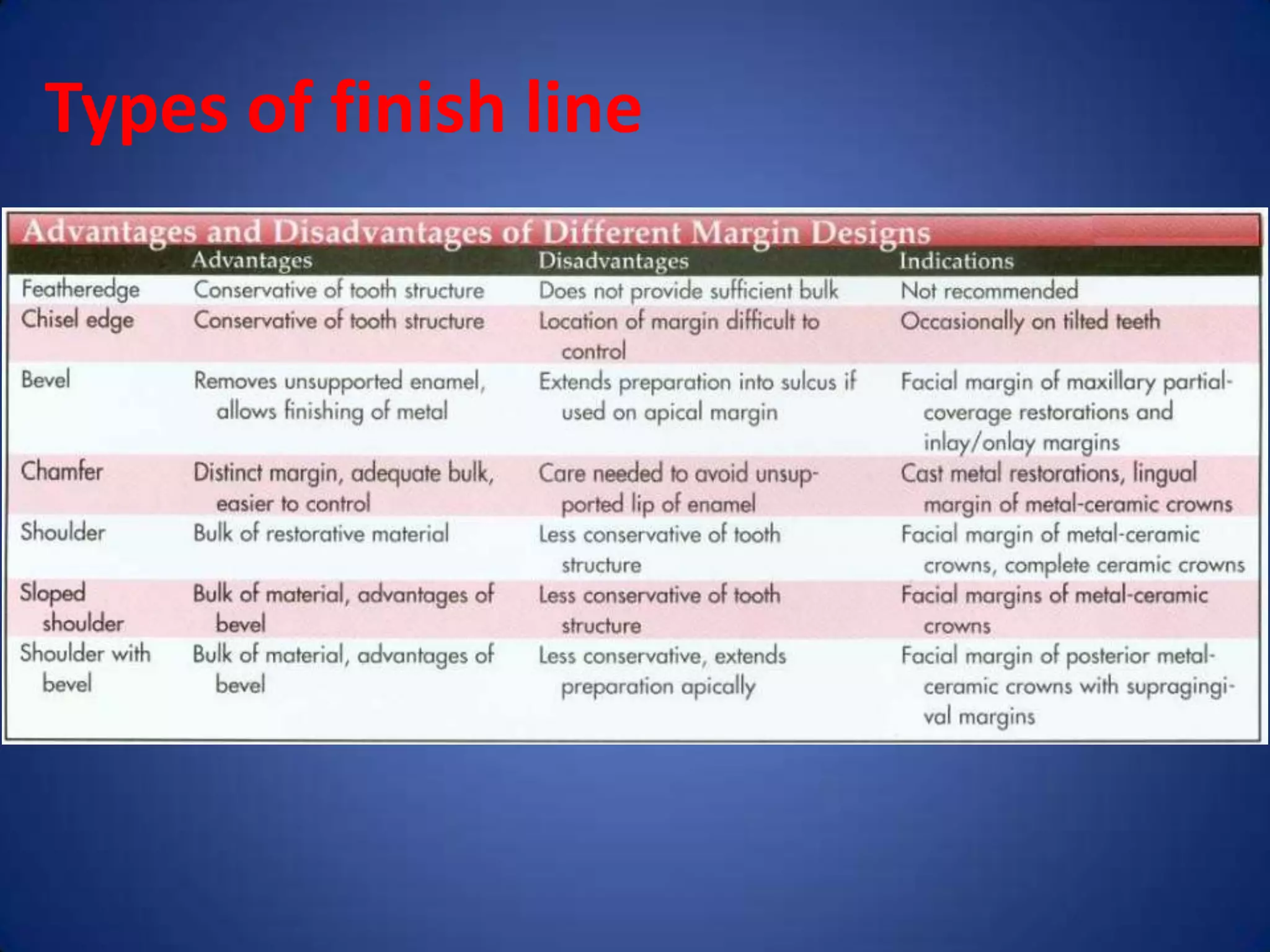
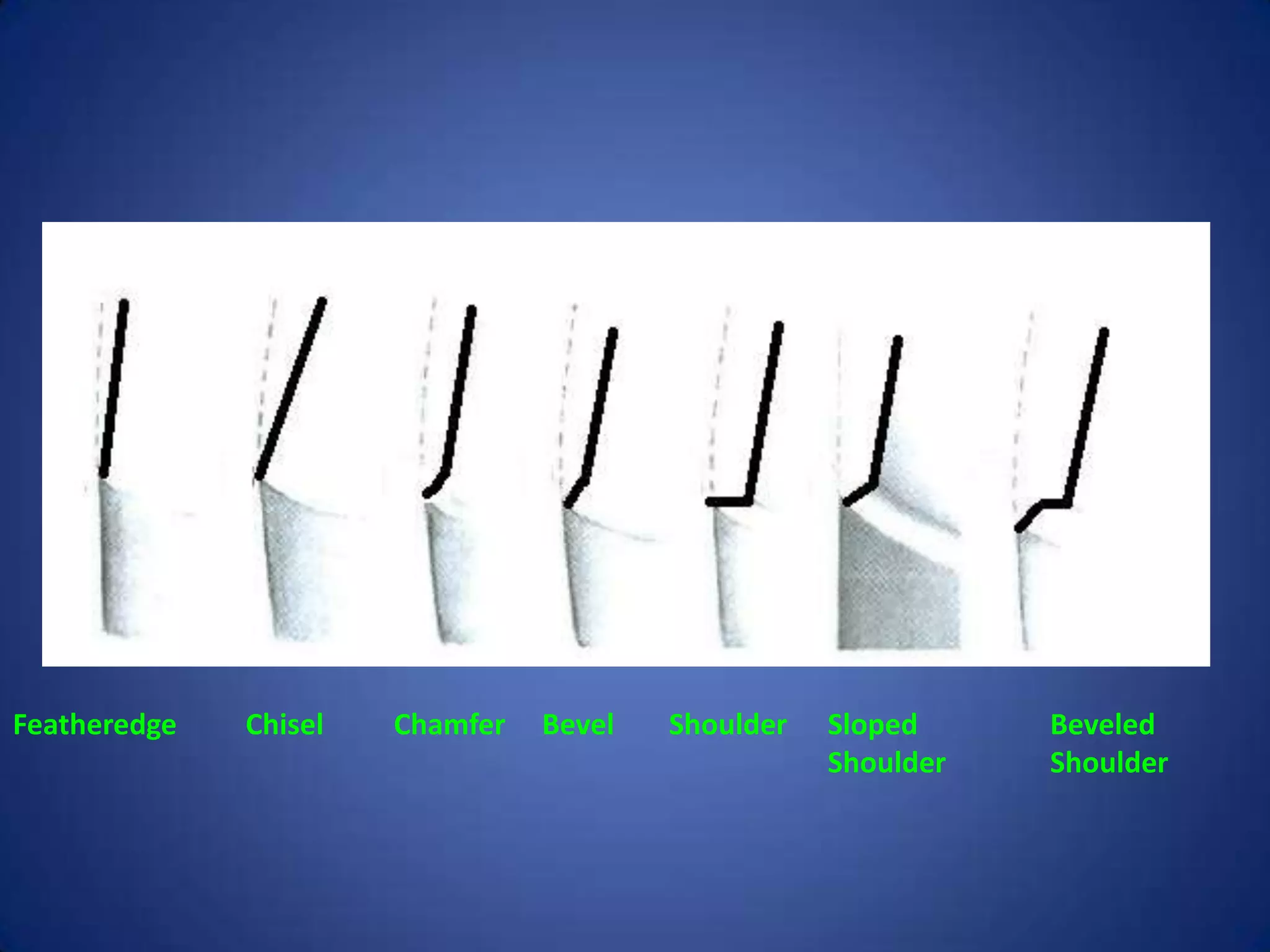
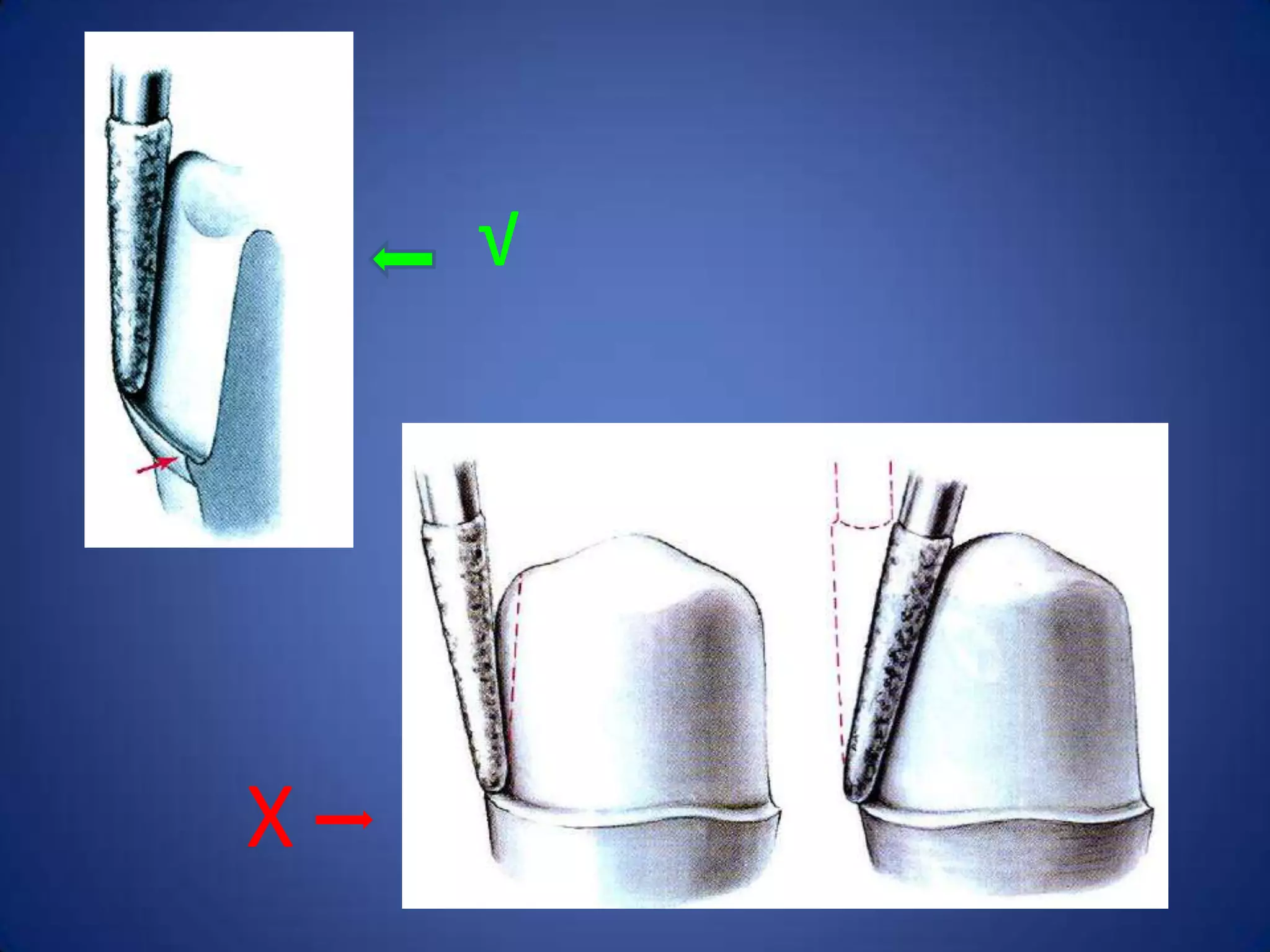

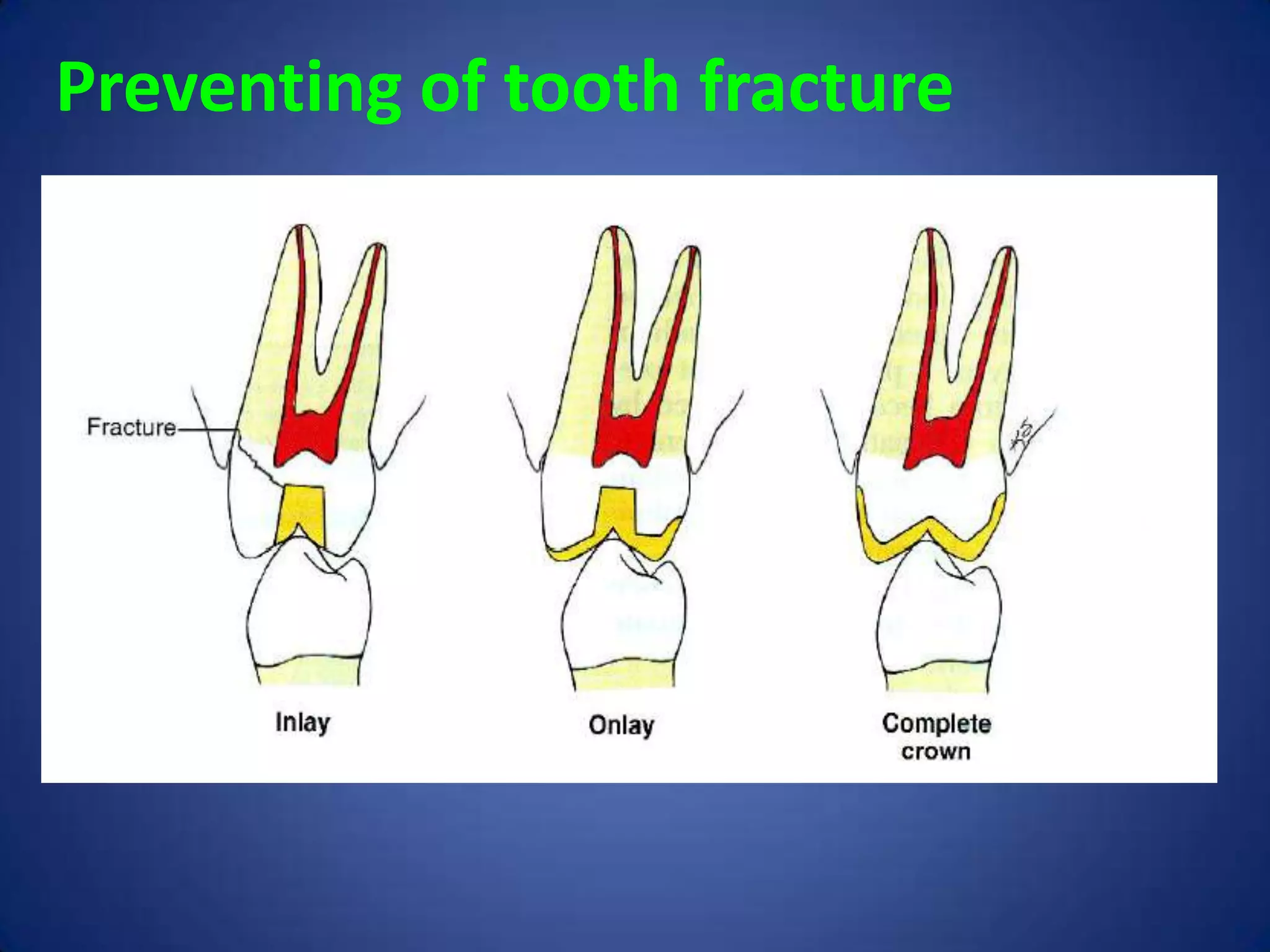

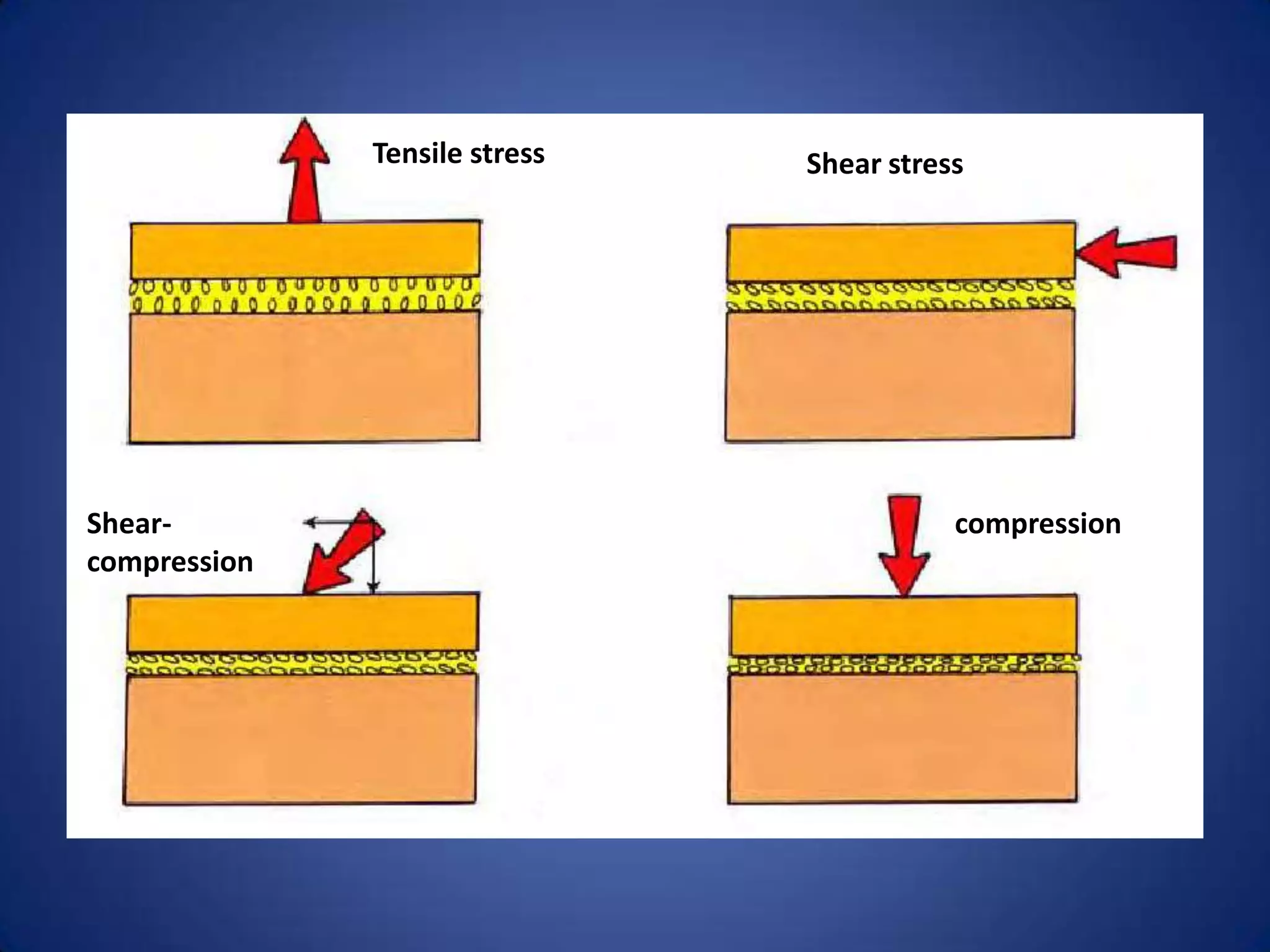
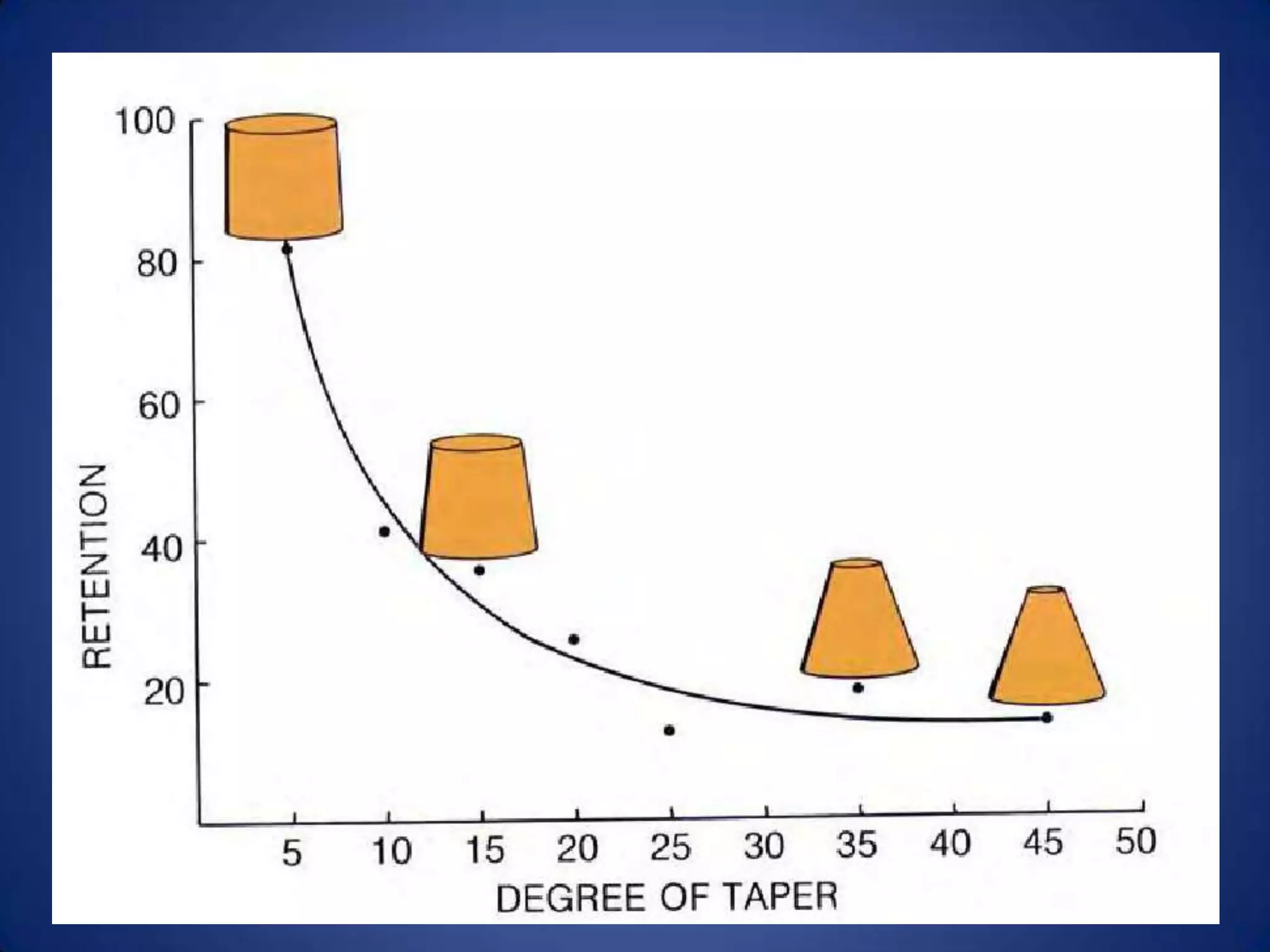

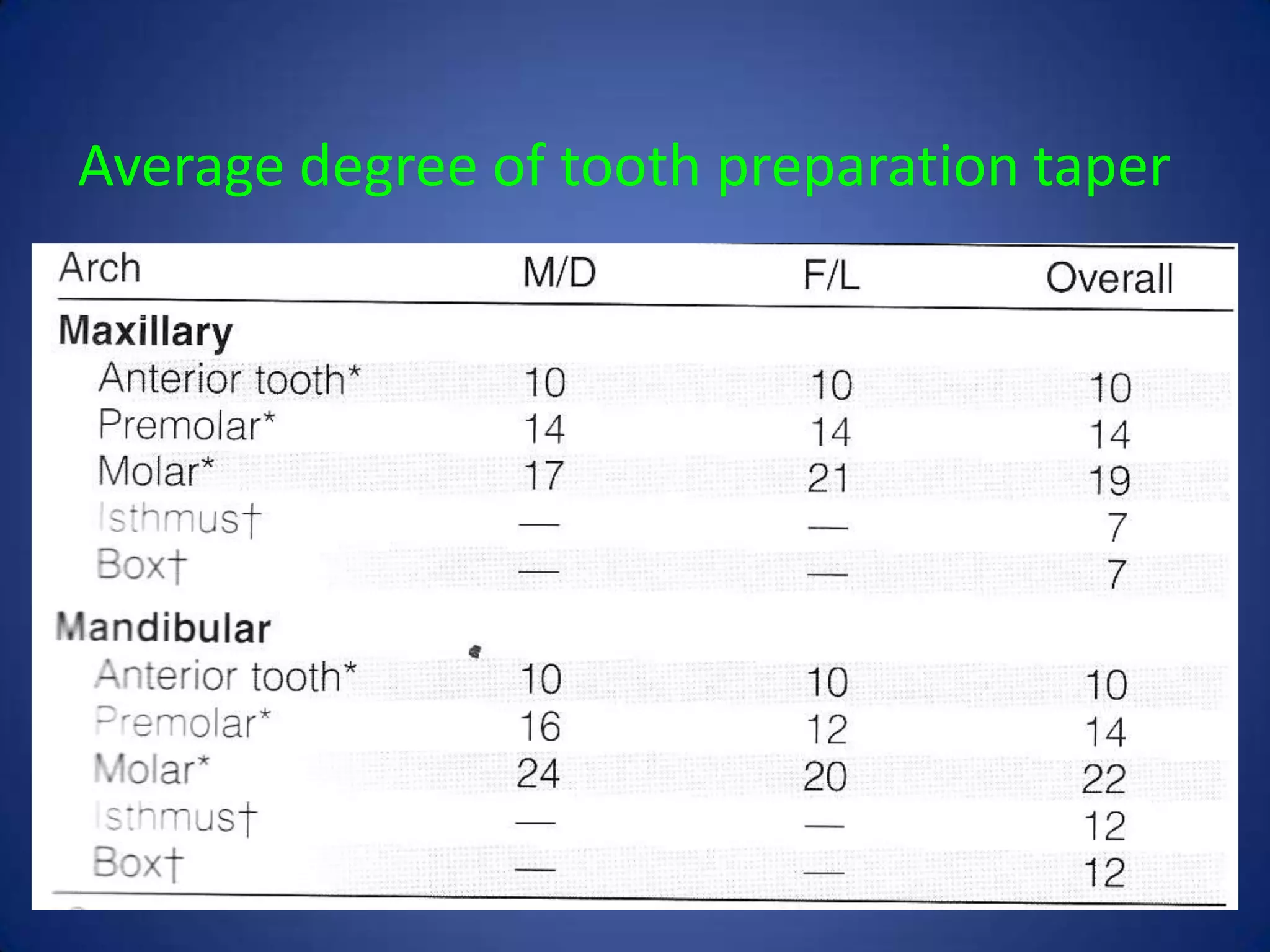
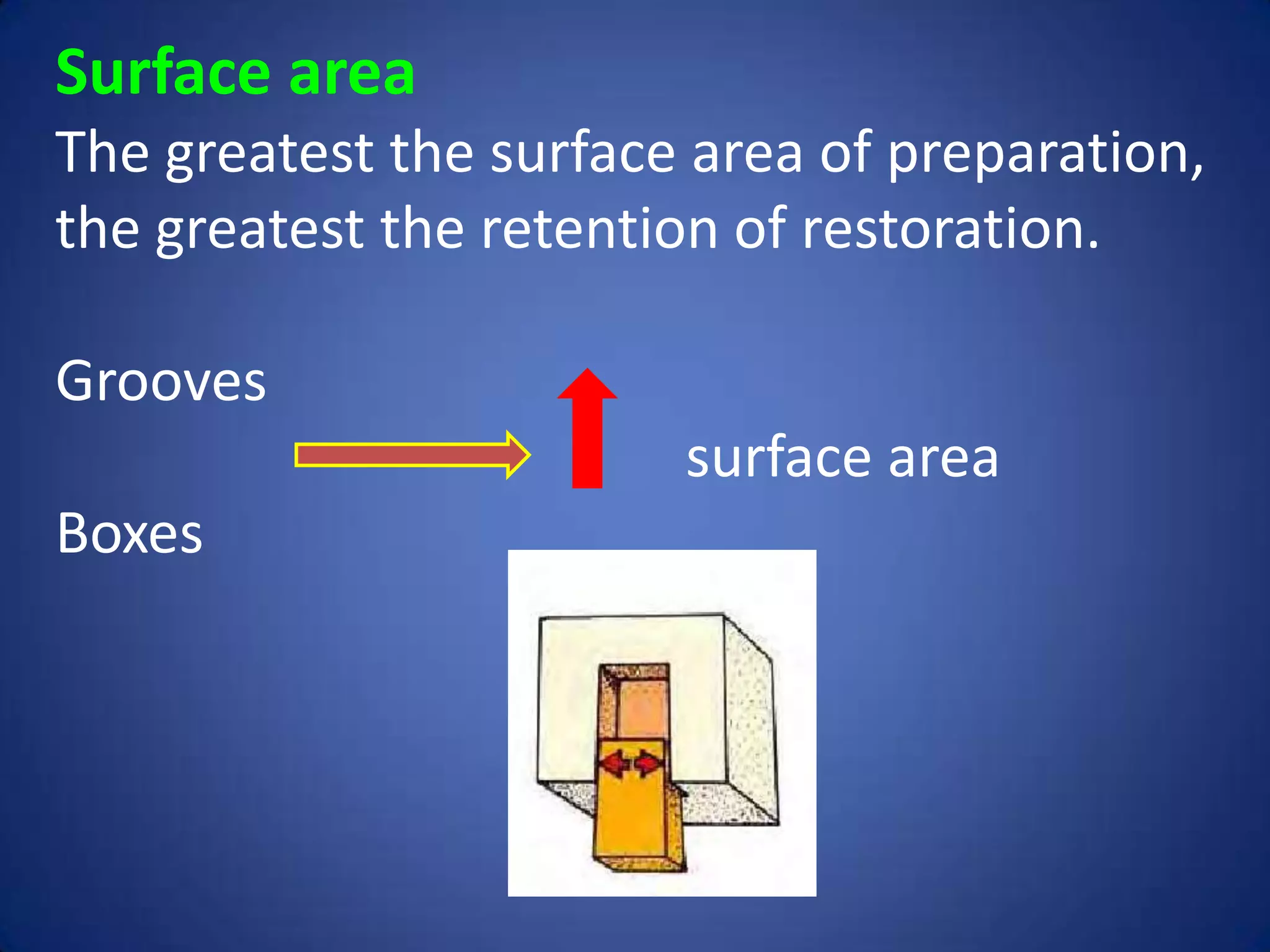
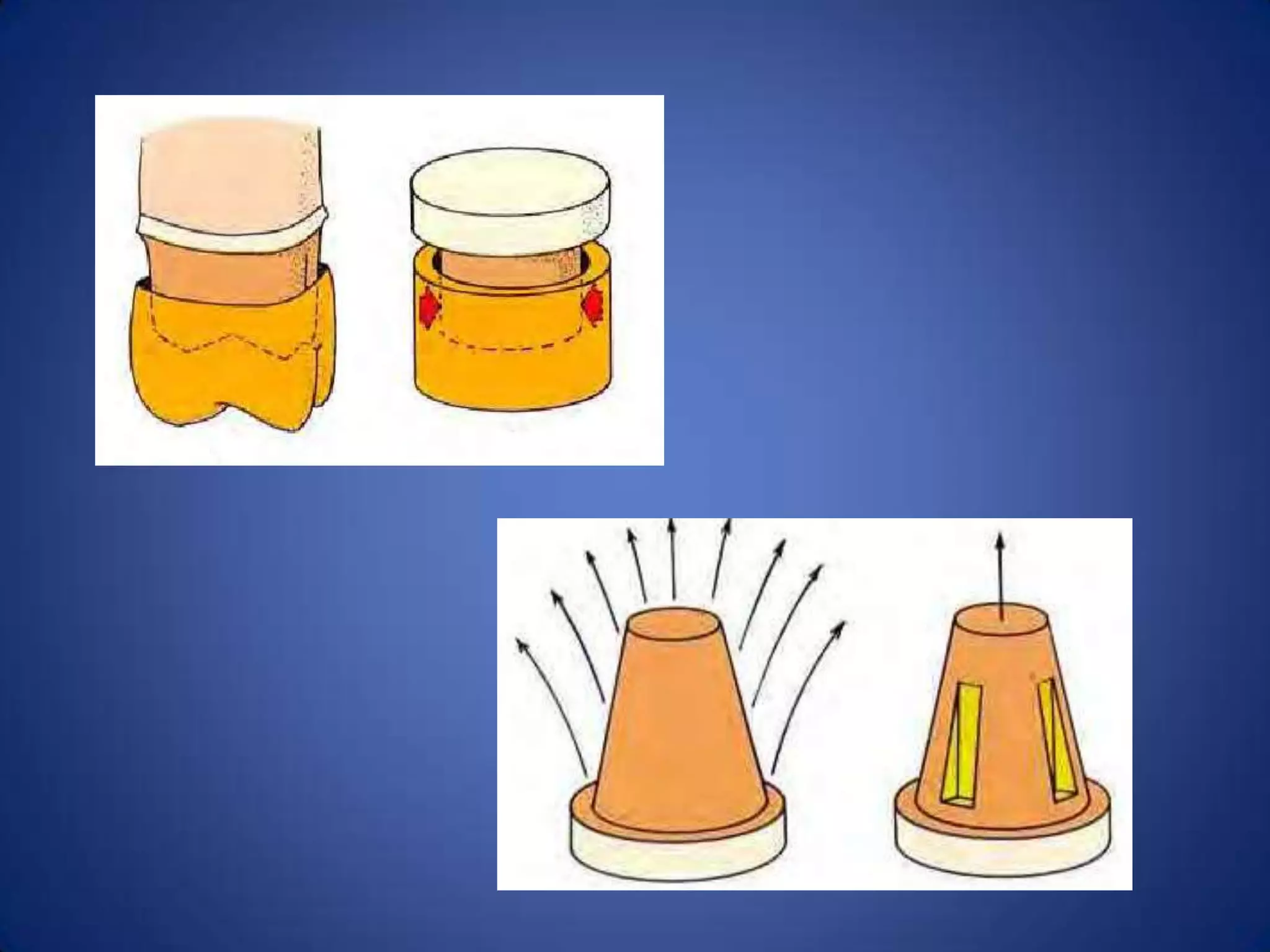
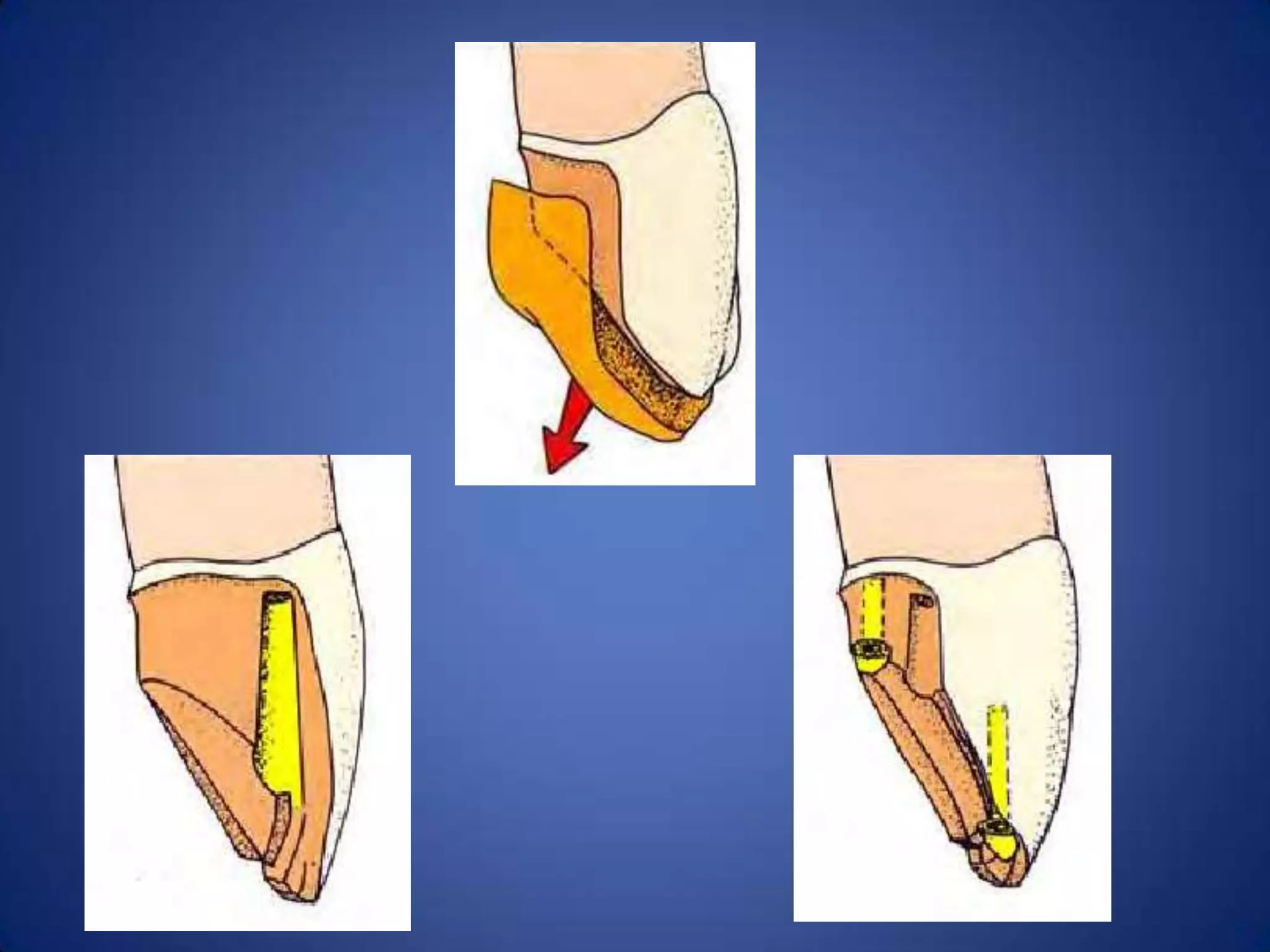
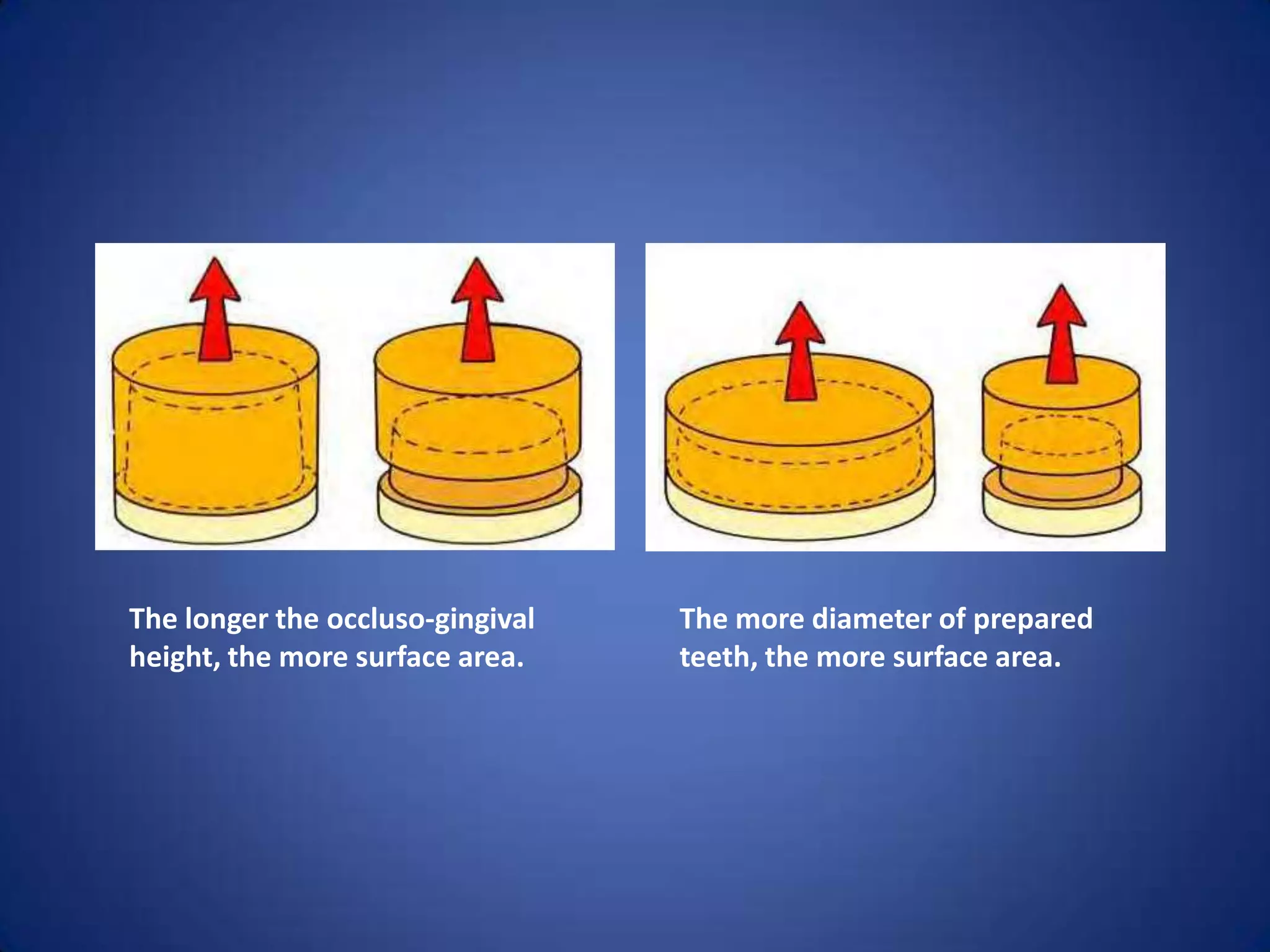
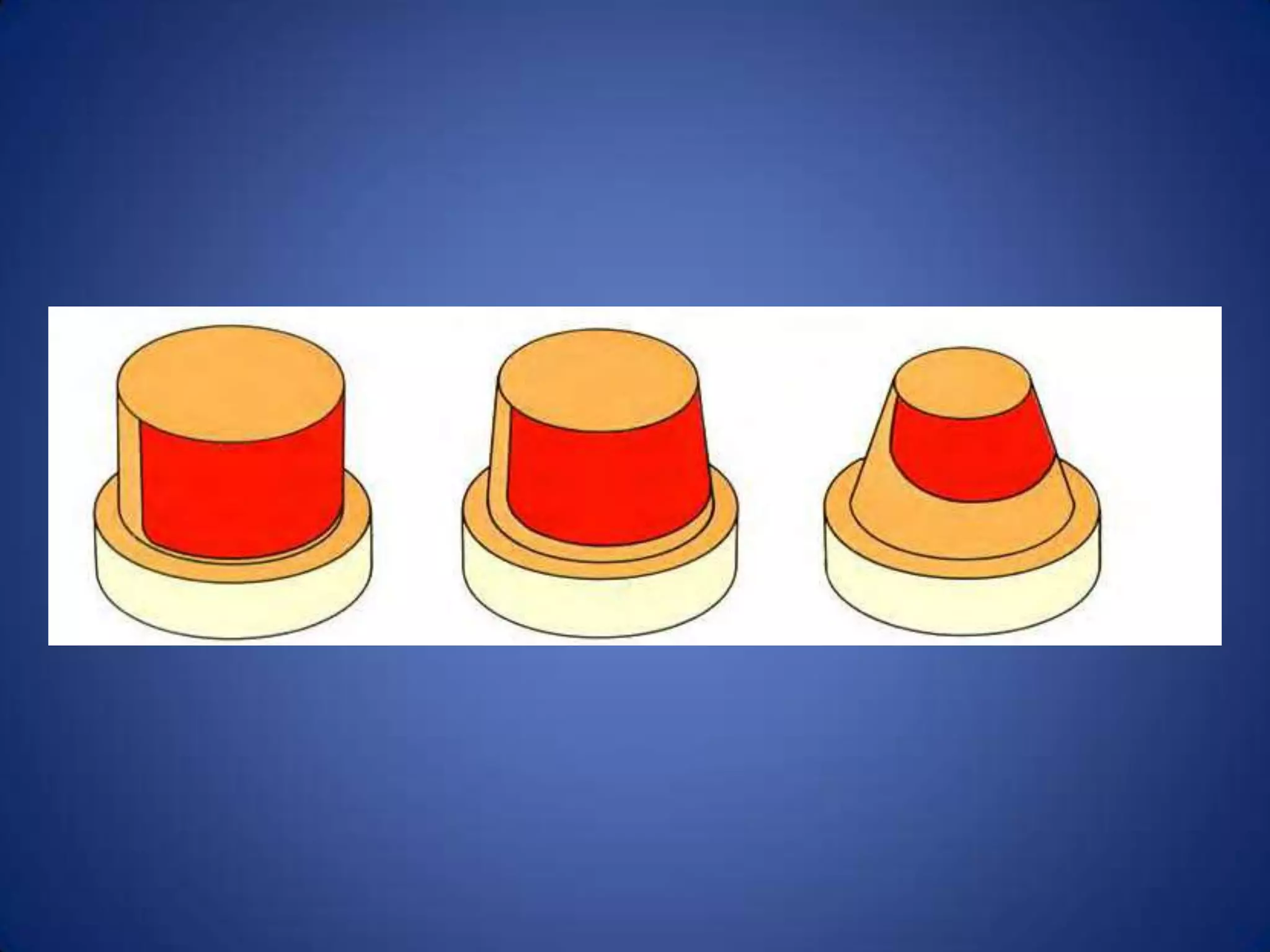
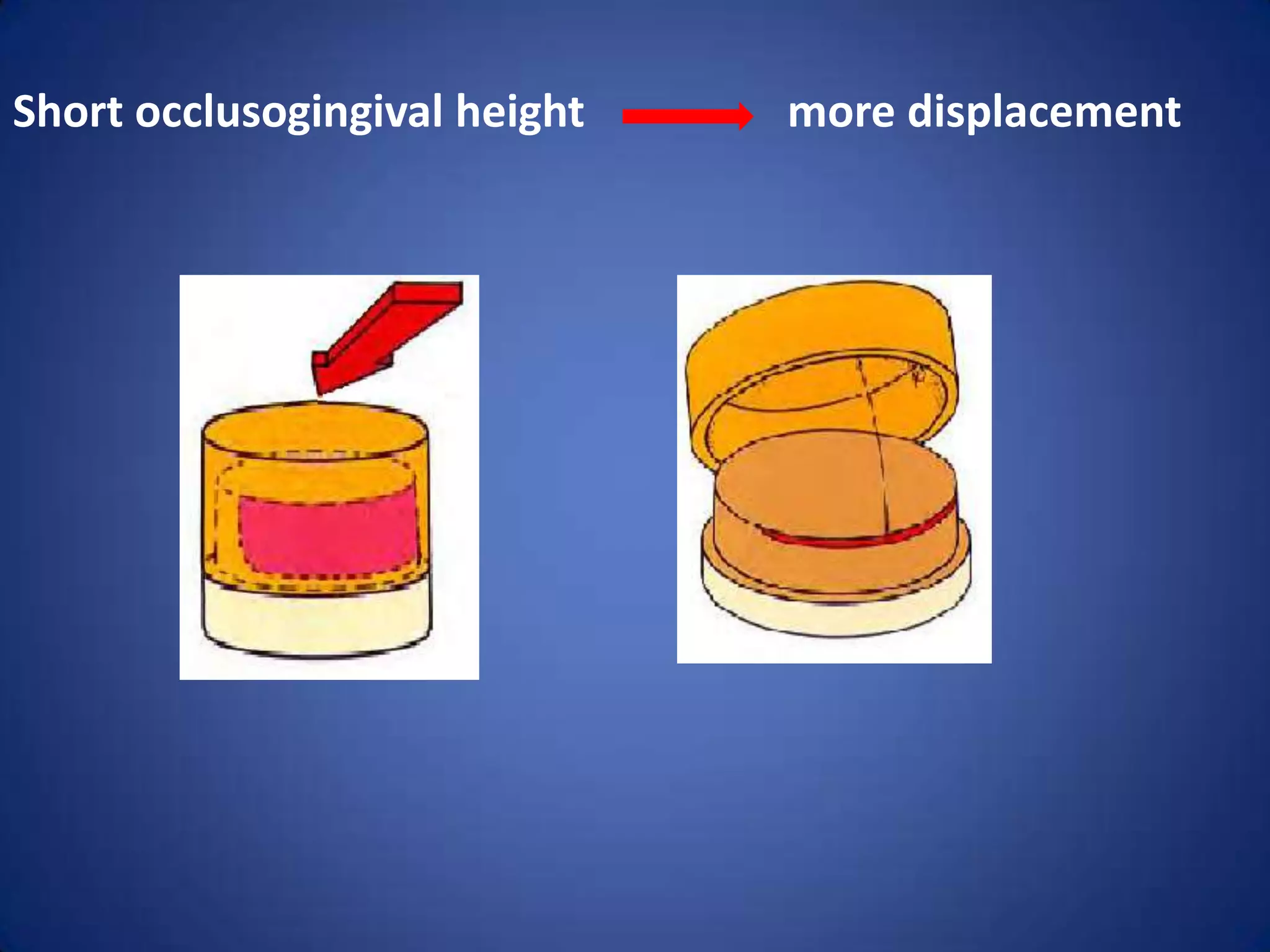
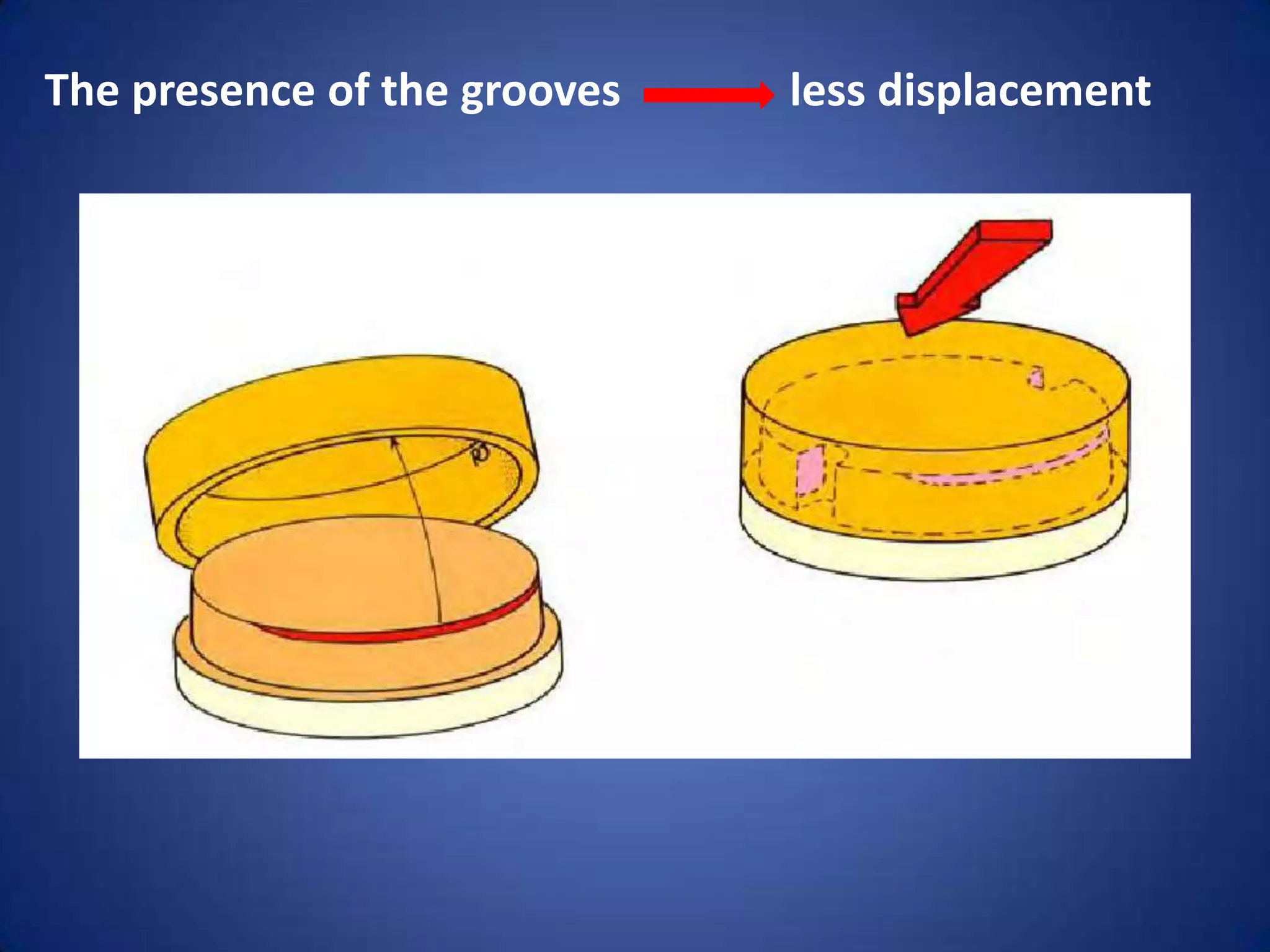
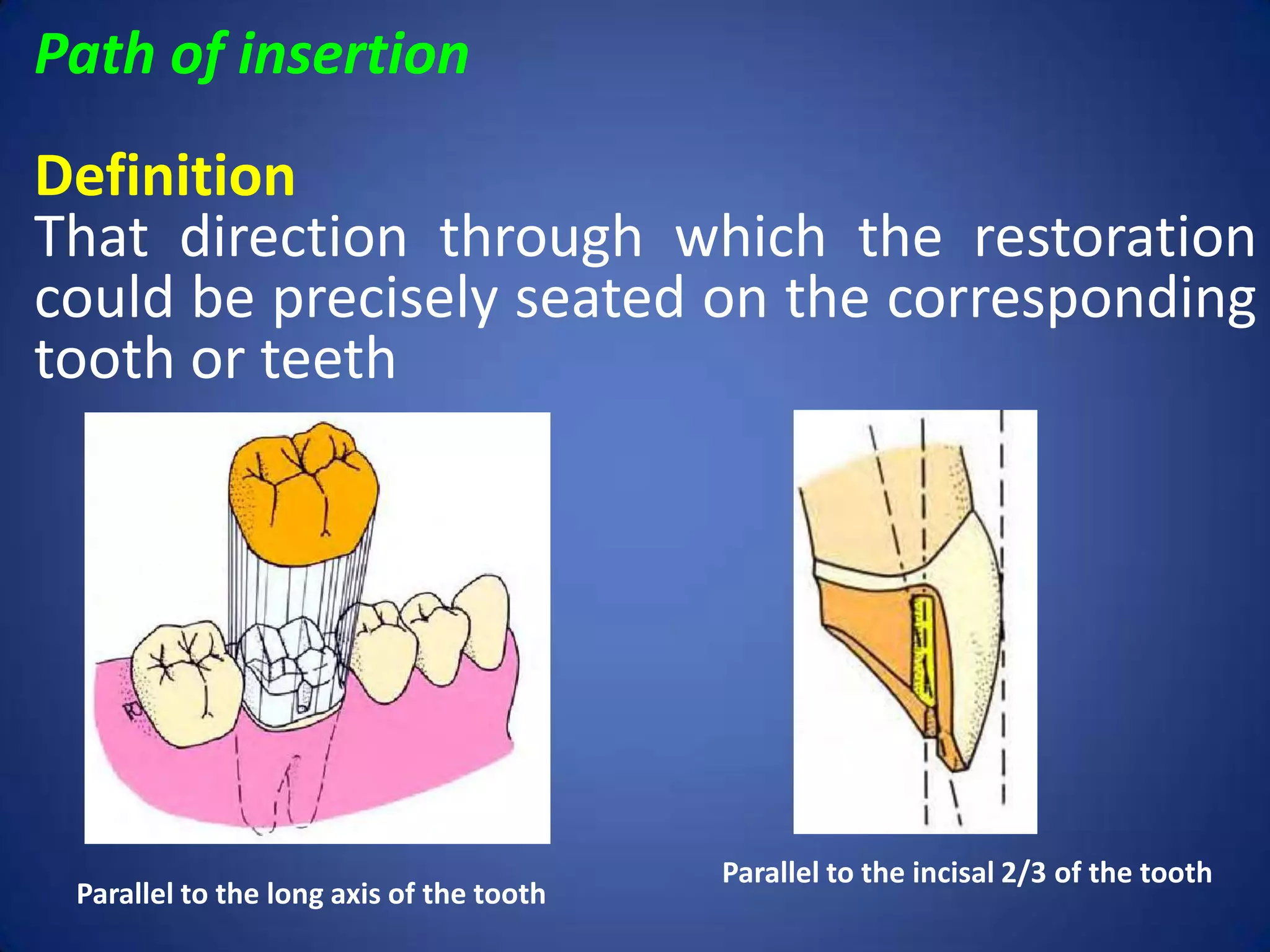
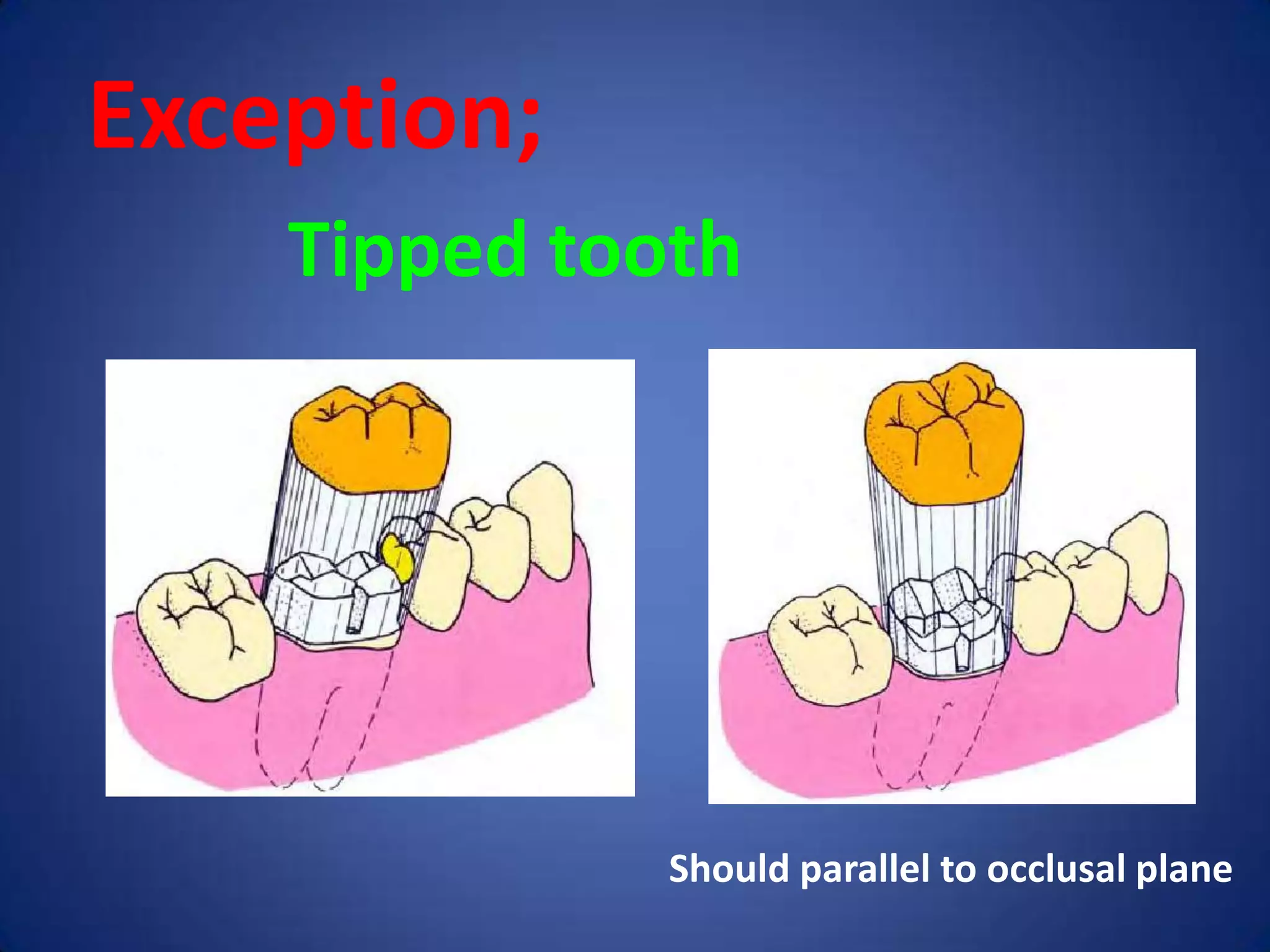
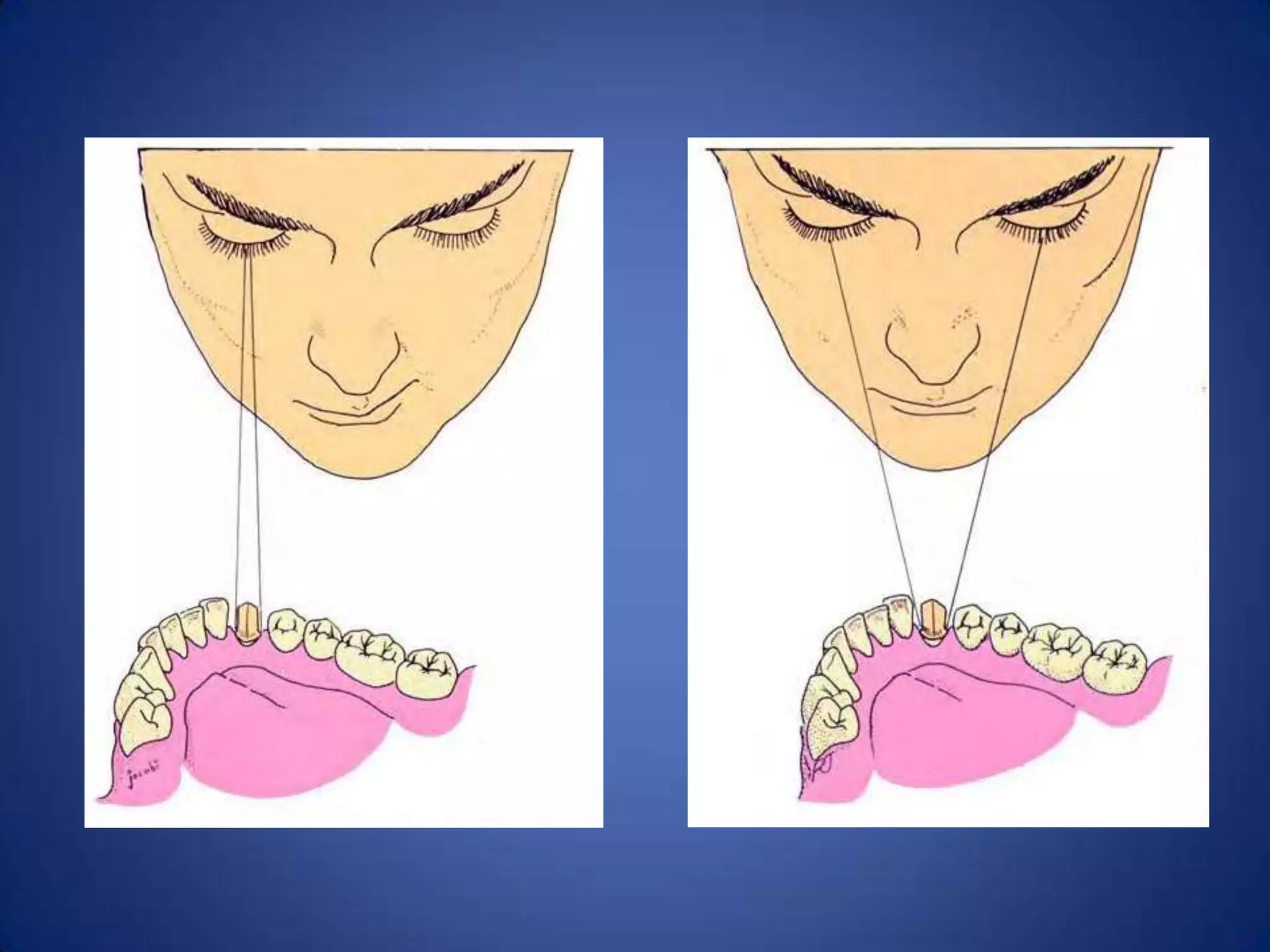
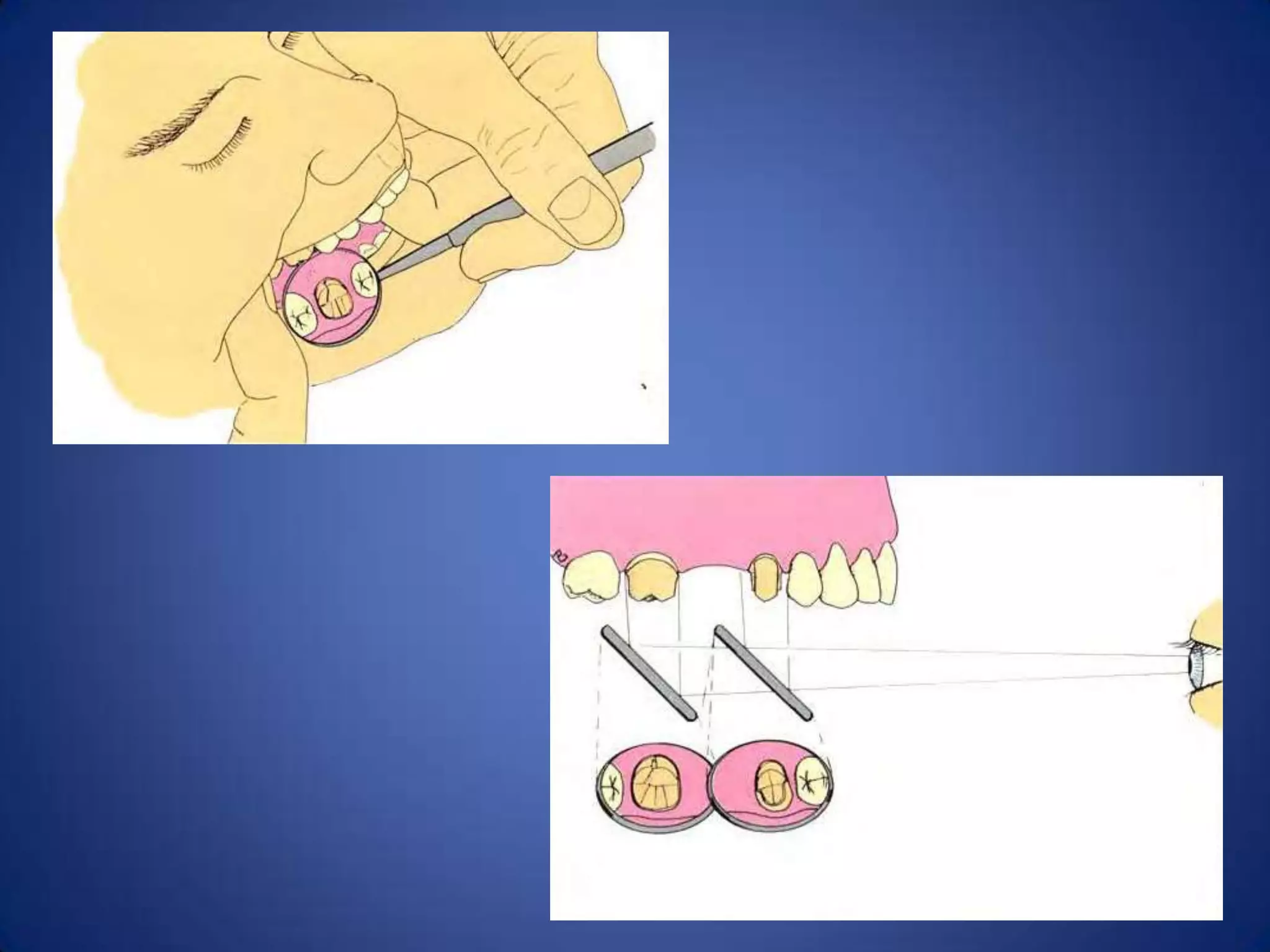
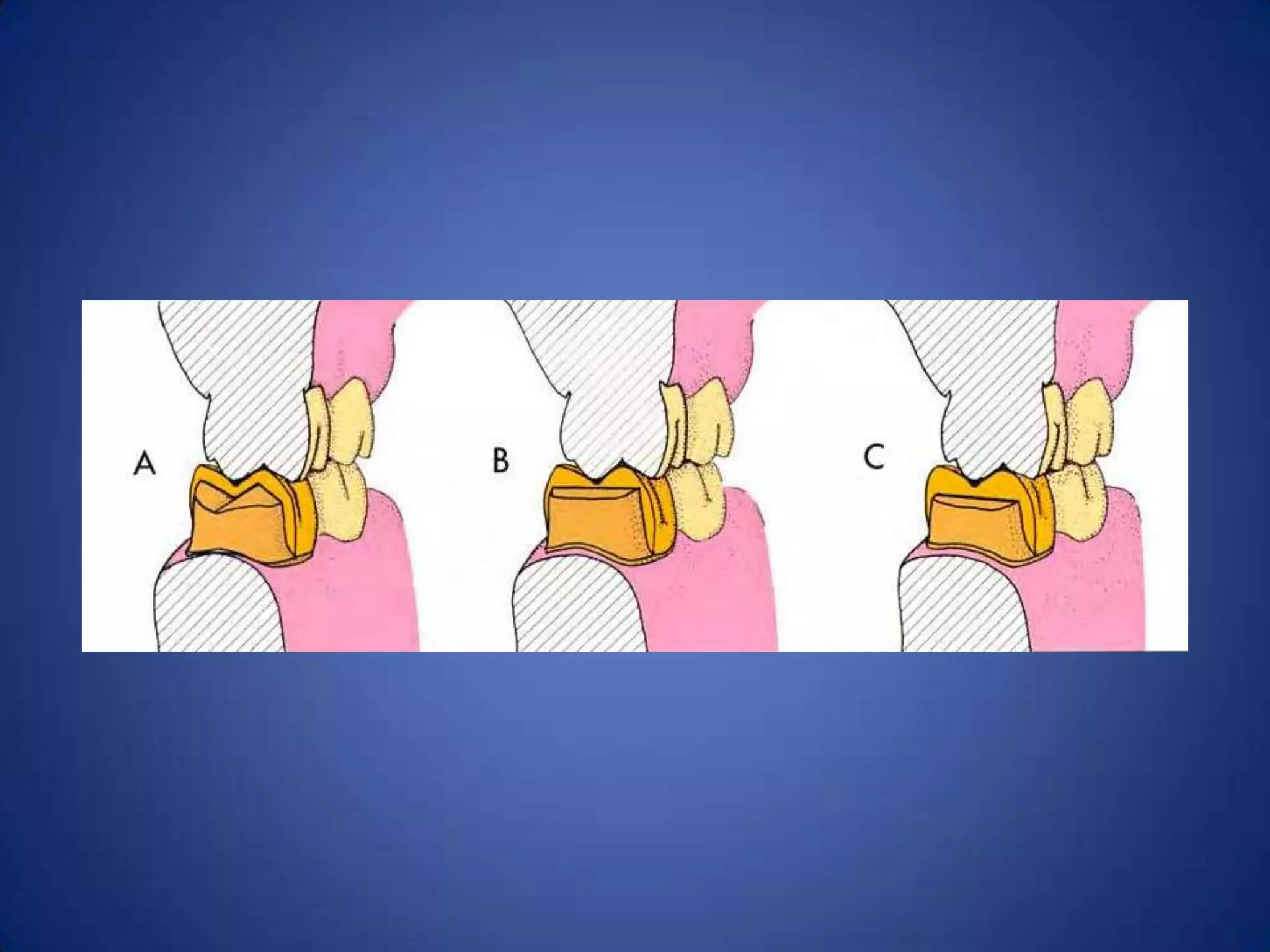
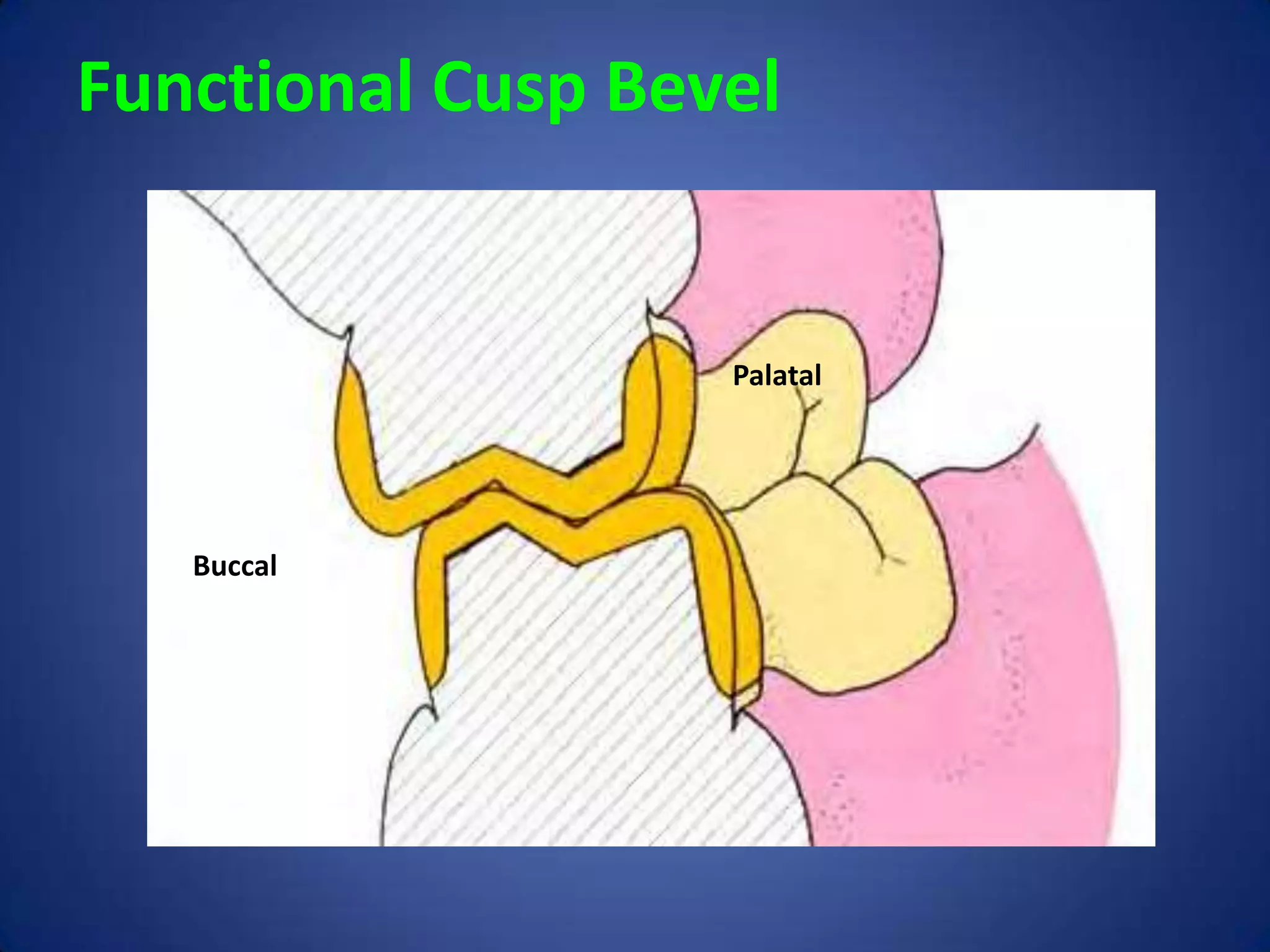
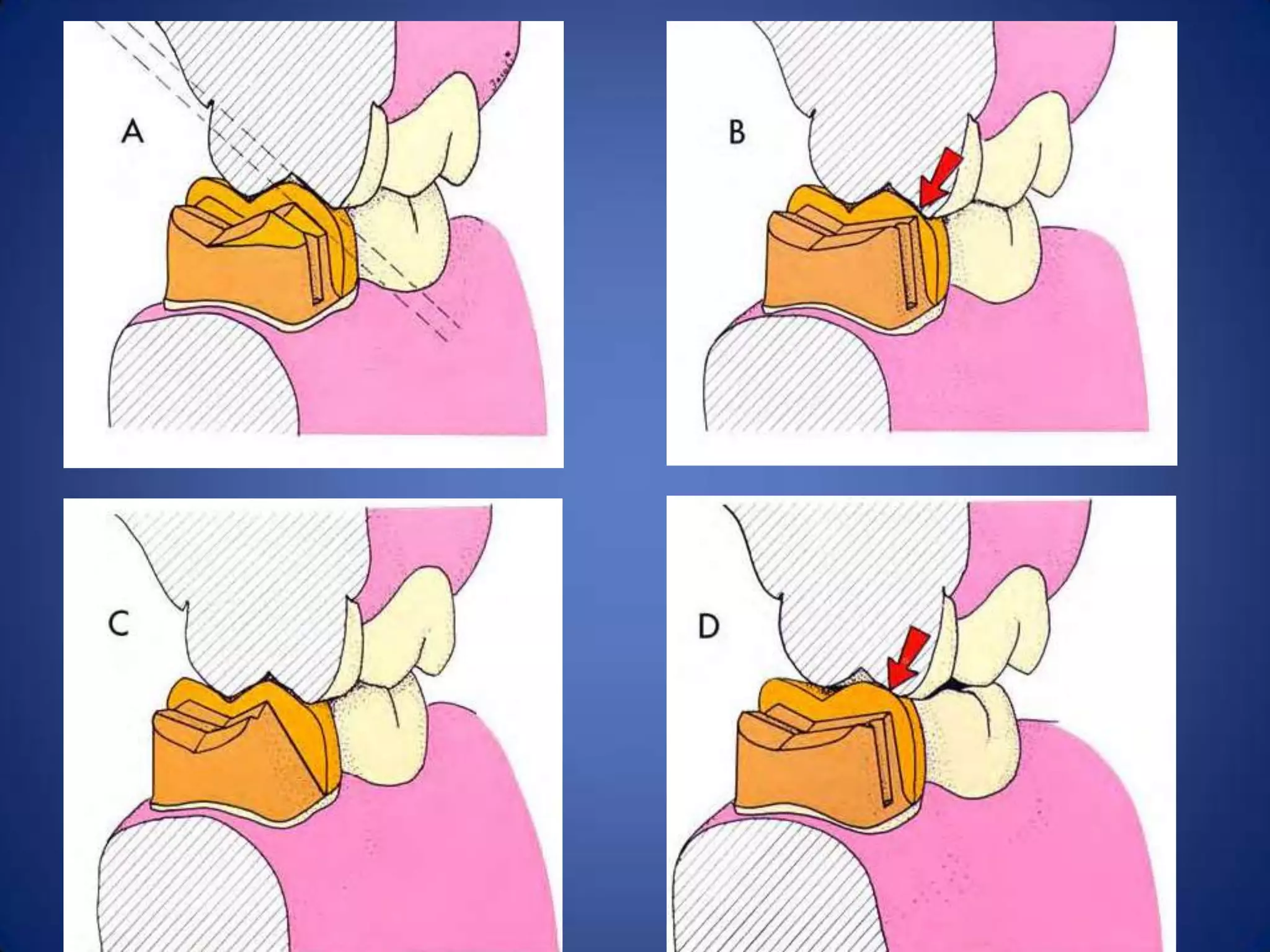
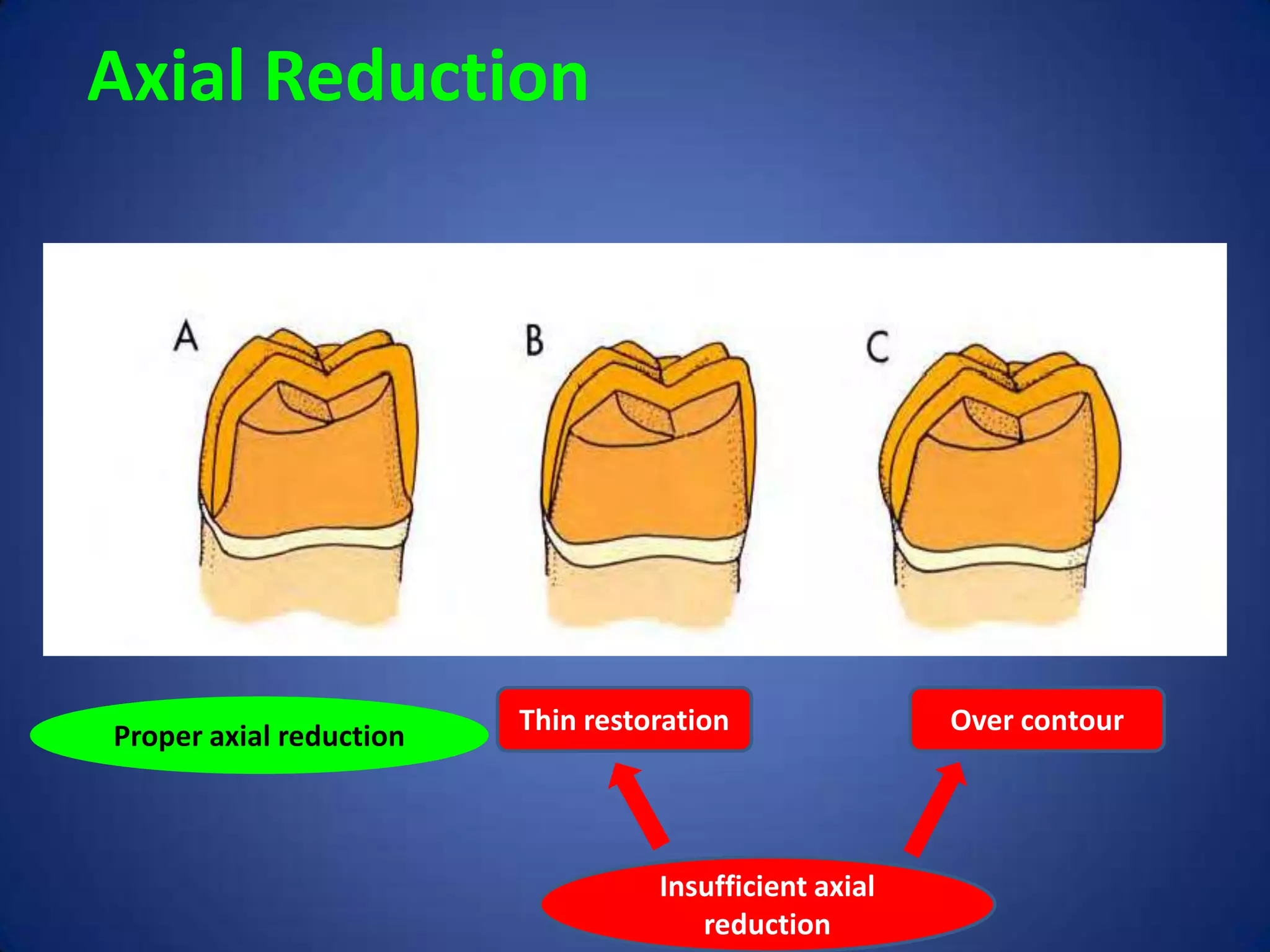



The document discusses principles of tooth preparation for dental restorations. It covers biological considerations like preserving tooth structure, margin placement, and preventing pulp injury. Mechanical considerations include providing retention and resistance form to prevent restoration deformation or displacement. Ideal preparation taper is 2.5-6.5 degrees. Surface area and roughness increase retention while resistance depends on forces and preparation geometry. Margin types include featheredge, chamfer, bevel and shoulder. Occlusal and axial reduction are needed with functional cusp bevels. Esthetic results factor preparation for all-ceramic, metal-ceramic or partial coverage restorations.





































































































