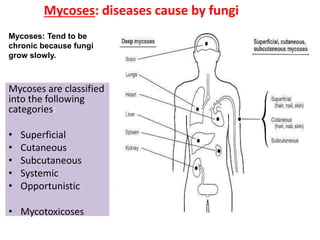
Mycoses: diseases causeby fungi
Mycoses are classified
into the following
categories:
• Superficial
• Cutaneous
• Subcutaneous
• Systemic
• Opportunistic
• Mycotoxicoses
Mycoses: Tend to be
chronic because fungi
grow slowly.
2.
Superficial mycoses
• Prevalentin tropical climates.
• Are fungal infections confined to the outer most dead layers
of skin, hair and nails
• do not penetrate deeper tissues
• Do not elicit a cellular response from the host.
• Infections are generally painless.
• No inflammation
• symptoms - discoloration, scaling, or de-pigmentation of the
skin.
• Superficial mycoses
– Black piedra
– White piedra
– Pityriasis versicolor
– tinea nigra
3.
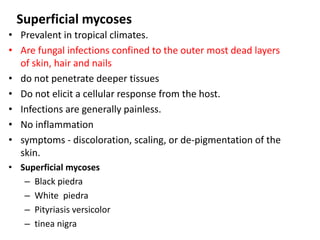
Superficial mycoses
Piedra isa fungal infection of the hair,
characterized by the presence of stony
hard nodules along the hair shaft
a) Black Piedra
• This disease is characterized by small
dark nodules seen on the hair shaft.
• Caused by Piedraia hortai
• The lesion is very discrete,
surrounds the hair shaft and is dark
brown.
4.
Superficial mycoses
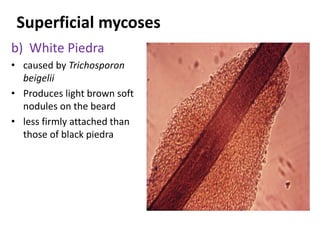
b) WhitePiedra
• caused by Trichosporon
beigelii
• Produces light brown soft
nodules on the beard
• less firmly attached than
those of black piedra
5.
Superficial mycoses
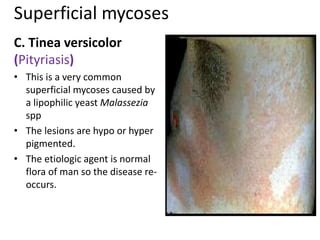
C. Tineaversicolor
(Pityriasis)
• This is a very common
superficial mycoses caused by
a lipophilic yeast Malassezia
spp
• The lesions are hypo or hyper
pigmented.
• The etiologic agent is normal
flora of man so the disease re-
occurs.
6.
Superficial mycoses
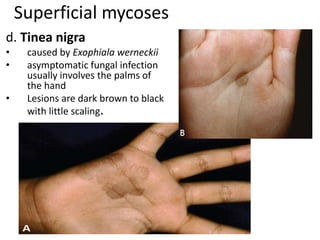
d. Tineanigra
• caused by Exophiala werneckii
• asymptomatic fungal infection
usually involves the palms of
the hand
• Lesions are dark brown to black
with little scaling.
7.
Laboratory Diagnosis
Direct Examination
•Scales should be scraped from the fawn colored macules with
a scrapler and mounted directly on a slide in a drop of 10%
potassium hydroxide
Culture and identification
• Specimen from lesions should be inoculated on sabouraud’s
dextrose agar (SDA) plate or slants at room temperature and
held for 3 weeks before being discarded
8.
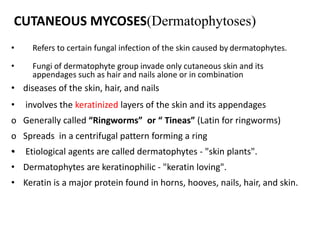
CUTANEOUS MYCOSES(Dermatophytoses)
• Refersto certain fungal infection of the skin caused by dermatophytes.
• Fungi of dermatophyte group invade only cutaneous skin and its
appendages such as hair and nails alone or in combination
• diseases of the skin, hair, and nails
• involves the keratinized layers of the skin and its appendages
o Generally called “Ringworms” or “ Tineas” (Latin for ringworms)
o Spreads in a centrifugal pattern forming a ring
• Etiological agents are called dermatophytes - "skin plants".
• Dermatophytes are keratinophilic - "keratin loving".
• Keratin is a major protein found in horns, hooves, nails, hair, and skin.
9.
Cutaneous mycosis cont’d…
Modeof transmission
• Infection is transmitted by direct contact or contact with
infected hair (hair salon) or cells (nail files, shower floors).
• Transmission of dermatophytic infection enhanced by
conditions of high moisture and sweating, and retention of
moisture increases the possibility of contracting infections.
10.
Clinical manifestations ofringworm infections are
called different names on basis of infection sites
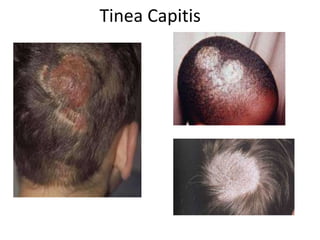
• tinea capitis - ringworm infection of the head, scalp,
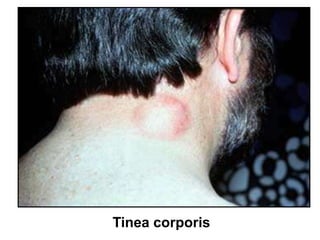
• tinea corporis - ringworm infection of the body (smooth skin)
• tinea cruris - ringworm infection of the groin (jock itch)
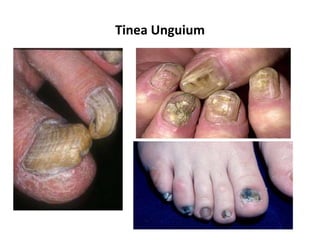
• tinea unguium - ringworm infection of the nails
• tinea barbae - ringworm infection of the beard
• tinea manuum - ringworm infection of the hand
• tinea pedis - ringworm infection of the foot (athlete's foot)
Diagnosis of dermatophytes
•Note the symptoms.
• Note the kind of tissue attacked
1. Direct Microscopy--- 10 % KOH
– KOH digest the keratin--- and enable the fungal elements to
be seen clearly
– Not sensitive
2. culture – Sabouraud Dextrose Agar (SDA
Dermatophyte Test medium (DTM)—selective medium
• SDA,
• cycloheximide,
• Antibiotic, phenol red
18.
KOH preparation
• areused in the initial examination of keratinized tissue
suspected of fungal infection.
Principle
• Fungal elements may be obscured by skin, hair, or nail tissue.
• KOH (20%w/v) dissolves keratin in skin, hair or nail specimens,
facilitating the observation of the organism’s morphology.
19.
Treatment
Skin infections
– Infectedskin may be treated with topical application of
antifungal agents miconazole and clotrimazole
– Refractory lesions oral griseofulvin and itraconazole,
terbinafine
Infections of hair and nails
– usually require systemic ( oral) therapy
20.
Subcutaneous mycoses
Fungalinfections beneath the skin- Subcutaneous tissues
dermis of the skin, deep tissues or bone.
• Causative organisms reside in the soil and in decaying or live
vegetation
• Almost always acquired through traumatic lacerations or
puncture wounds
• Common among those who work with soil and vegetation and
have little protective clothing--- occupational
• Not usually transmitted humans to humans
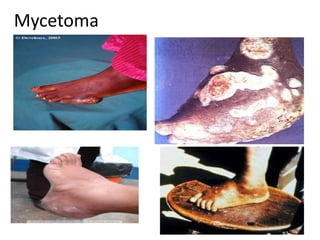
• Mycetoma
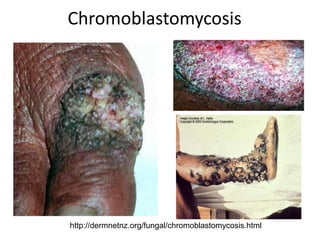
• Chromoblastomycosis
• Sporotrichosis
Sporotrichosis
• chronic infectioncaused sporotrichum schenckii- dimorphic
fungus
• Sporotrichum schenckii exists in nature where it has been isolated
from soil, wood and plants.
• Human bieng and animals become infected by contact with
contaminated materials at the time of an injury to the skin of
hand, arm and leg, and inhalation.
• The infection is an occupational hazard - farmers
• It is commonly known as “rose gardener’s”disease
• Yeast travel along lymphatics
• Elicit mixed pyogenic/ granulomatous reaction
• Granauloma ulcer at a puncture skin usually a thorn prick and may
produce secondary lesions along draining lymphatics
26
Systemic / Deep/ Endemic Mycoses
• Caused by true pathogens (infect both healthy and
immunocompromised patient)
• Caused by endemic dimorphic fungi
• Dimorphic:-
• exist in a mould form or in nature or in the
laboratory at 250C to 300c and
• in yeast in tissues or in culture media in laboratory at
370C
• Endemic/occur only in certain regions of the world
27.
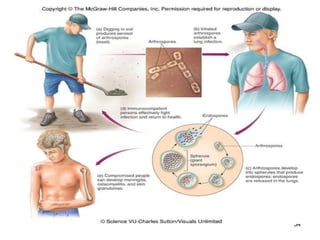
Systemic mycosis… con’t
•Infection is commonly acquired by inhalation of spores from the
environment and may spread form the lung to other sites
• Inhalation pulmonary inf. dissemination
• Most infections are asymptomatic or self-limiting
• In immune-compromised hosts, infections are more severe and
often fatal
Clinical pictures
• Primary infection:
– Fever, chest pain, cough, weight loss
– Nodular lesions in lungs
• Secondary (disseminated) infection:
HISTOPLASMOSIS
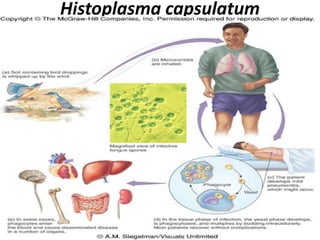
• Caused by---Histoplasma capsulatum
• Dimorphic soil organism
• The fungus is found in soil, in decaying plant materials, but
especially in droppings of bats and some birds
• Transmission: Inhalation of air-borne asexual spores (conidia)
• Spores transform to yeast in lung, elicit cellular immunity as per
TB--- clinically mimics TB
• An intracellular mycoses of the reticuloendothelial system,
attacking lungs, liver, spleen, bone marrow
• skin test reactivity (histoplamin)
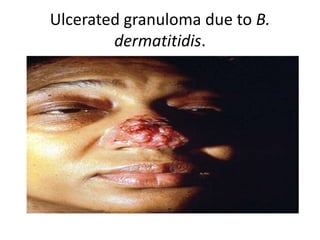
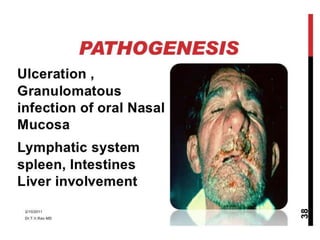
Blastomycosis
• Sub-acute &chronic fungal infection.
• Etiologic agent: Blastomyces dermatitidis
• It affects lungs, skin and bone
• Infection--- inhalation of spores
• Pathophysiology_-- Spores transform into yeast in lung,
disseminate
• Causes --primary pulmonary blastomycosis and cutanous
• The more common is the secondary form resulting from
dissemination from a lung lesion which manifests as nodules,
gummata, abscesses and ulcers in various regions of the body
• Later nodular, verrucous and ulcerous lesions develop
33
Coccidioidomycosis
• Caused byC. immitis
• C.immitis is found in soil --enhanced by bat and rodent dropping.
• C.immitis is probably the most virulent
• Inhalation of a few arthroconidia produce 10 infection which result
asymptomatic or a self limited flue like illness
• Spores transform to spherules in lung, elicit cellular immunity as
per TB
• Like syphilis and tuberculosis coccidiodomycosis causes a wide
varieties of lesions and has been called the great imitator.
• Disseminated infection (Extra pulmonary infection) includes skin,
soft tissues, bones, joints, and meninges
• Skin test reactivity (coccoidin)
35
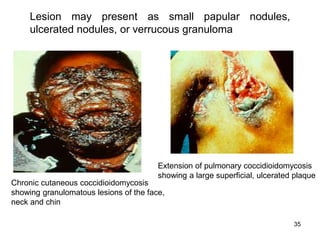
Chronic cutaneous coccidioidomycosis
showinggranulomatous lesions of the face,
neck and chin
Extension of pulmonary coccidioidomycosis
showing a large superficial, ulcerated plaque
Lesion may present as small papular nodules,
ulcerated nodules, or verrucous granuloma