More young people in Canada are visiting EDs because of drinking alcoholΔρ. Γιώργος K. Κασάπης
More people are visiting emergency departments after drinking alcohol, a new study finds. Researchers looked at more than 765,000 ED visits in Ontario, Canada’s largest province, and found a 175% increase in such visits between 2003 and 2016 among 25- to 29-year-olds. That spiked to a 240% increase in alcohol-related ED visits for young women, who were also more likely than men to be under Canada’s legal drinking age of 19. For both young men and women, visiting the ED for alcohol-related problems also led to more hospital admissions than other types of ED visits. Other countries, including the U.S., have experienced similar increases in alcohol-related visits to the ED, the authors behind the new study write, urging more research into the reasons behind the growing trend.
Preventable Medical Errors is the 3rd leading cause of death in America. US hospitals are penalized for poor quality. Doctella.com helps hospitals improve patient safety, education, education and empowerment.
The authors behind a new paper are encouraging good medical billing practices, arguing that it’s a mark of quality health care. The information medical bills contain and what tactics companies use to collect payment can vary, but the authors outline five metrics by which to judge medical bills.
Among them: Bills of high quality would provide patients with an itemized and understandable list of services; would allow patients to easily contact a representative to clarify or contest their bill; and wouldn’t involve any “surprise” charges
Sophie Peresson
Director, Pharmaceuticals & Healthcare Programme - Transparency International UK
Sophie Peresson is the Director of Transparency International’s Pharmaceuticals and Healthcare Programme (PHP). http://www.transparency.org.uk/our-work/pharmaceuticals-healthcare-programme/
The Programme has been set up, with a purpose to achieve genuine change in the pharmaceutical & healthcare sector through reducing corruption and promoting transparency, integrity and accountability.
Sophie holds a Masters in Law from the Sorbonne University, a post-graduate degree from the School of Advanced International Studies (SAIS) Johns Hopkins University. She is currently completing an MSc in Global Health at the London School of Hygiene and Tropical Medicine.
She has over fifteen years’ experience of working in public health, working for influential international NGOs such as the Red Cross and Marie Stopes International. Her experience spans both communicable and non-communicable diseases. She is an expert adviser to the European Institute for Women’s Health (EIWH) and has held several board positions. She is also a contributor to the Global Burden of Disease Study. She has a well-established track record in collaborating in international projects, research initiatives and has been on the steering committee of several influential publications, e.g. The Diabetes Policy Puzzle.
More young people in Canada are visiting EDs because of drinking alcoholΔρ. Γιώργος K. Κασάπης
More people are visiting emergency departments after drinking alcohol, a new study finds. Researchers looked at more than 765,000 ED visits in Ontario, Canada’s largest province, and found a 175% increase in such visits between 2003 and 2016 among 25- to 29-year-olds. That spiked to a 240% increase in alcohol-related ED visits for young women, who were also more likely than men to be under Canada’s legal drinking age of 19. For both young men and women, visiting the ED for alcohol-related problems also led to more hospital admissions than other types of ED visits. Other countries, including the U.S., have experienced similar increases in alcohol-related visits to the ED, the authors behind the new study write, urging more research into the reasons behind the growing trend.
Preventable Medical Errors is the 3rd leading cause of death in America. US hospitals are penalized for poor quality. Doctella.com helps hospitals improve patient safety, education, education and empowerment.
The authors behind a new paper are encouraging good medical billing practices, arguing that it’s a mark of quality health care. The information medical bills contain and what tactics companies use to collect payment can vary, but the authors outline five metrics by which to judge medical bills.
Among them: Bills of high quality would provide patients with an itemized and understandable list of services; would allow patients to easily contact a representative to clarify or contest their bill; and wouldn’t involve any “surprise” charges
Sophie Peresson
Director, Pharmaceuticals & Healthcare Programme - Transparency International UK
Sophie Peresson is the Director of Transparency International’s Pharmaceuticals and Healthcare Programme (PHP). http://www.transparency.org.uk/our-work/pharmaceuticals-healthcare-programme/
The Programme has been set up, with a purpose to achieve genuine change in the pharmaceutical & healthcare sector through reducing corruption and promoting transparency, integrity and accountability.
Sophie holds a Masters in Law from the Sorbonne University, a post-graduate degree from the School of Advanced International Studies (SAIS) Johns Hopkins University. She is currently completing an MSc in Global Health at the London School of Hygiene and Tropical Medicine.
She has over fifteen years’ experience of working in public health, working for influential international NGOs such as the Red Cross and Marie Stopes International. Her experience spans both communicable and non-communicable diseases. She is an expert adviser to the European Institute for Women’s Health (EIWH) and has held several board positions. She is also a contributor to the Global Burden of Disease Study. She has a well-established track record in collaborating in international projects, research initiatives and has been on the steering committee of several influential publications, e.g. The Diabetes Policy Puzzle.
The last thing you expect when you seek help from a medical professional is that they will cause you harm. If you or a loved one have suffered an injury or illness due to the negligence of a medical professional, you need to consider seeking legal assistance today. Contact a Salt Lake City medical malpractice lawyer Joseph Jardine at the Jardine Law Offices P. C.
Researchers call for a unified approach to preventing suicides and other self...Mrsunny4
Self-injury mortality (SIM), a composite of all methods of suicide and estimated non-suicide deaths from drug self-intoxication, has surpassed diabetes as the seventh leading cause of death in the United States, prompting researchers to call for a new unified approach to SIM prevention.
Senior Citizens need to have comprehensive medical evaluations that are readily available to emergency providers. Electronic Medical Recording is ideal for having much needed information at the proper person's finger tips. The hesitancy of primary care physicians to employ EMR/EHR systems places a heavy burden on emergency departments in the United States. Senior citizens often have special needs that are not readily known by first responders and in a crisis situations, the care provided is based on standard of care and not special needs. Innovative alternatives to the current data taking, storage and retrieval process.
Diabetes & Texas Medicaid Savings 11 01thoenner
Diabetes affects nearly 24 million people in the United States, an increase of more than 3 million in just two years. The Diabetes epidemic cost the U.S. economy more than $200 billion each year in medical expenses and lost productivity. This presentation outlines the challenges and proposes practical proven solutions aimed at improving outcomes while reducing the cost of treating Medicaid eligible Texans with diabetes.
SBIRT and SAMHSA's 8 Strategic Initiativessideponytail
Slides from a webinar held by the National SBIRT ATTC. Video is on TheIRETAChannel on Youtube: http://www.youtube.com/watch?v=f6NrKuGlGRs&feature=share&list=PLiML4AFpuB72LBaPShcu2yQv_WpsGY9a9
The last thing you expect when you seek help from a medical professional is that they will cause you harm. If you or a loved one have suffered an injury or illness due to the negligence of a medical professional, you need to consider seeking legal assistance today. Contact a Salt Lake City medical malpractice lawyer Joseph Jardine at the Jardine Law Offices P. C.
Researchers call for a unified approach to preventing suicides and other self...Mrsunny4
Self-injury mortality (SIM), a composite of all methods of suicide and estimated non-suicide deaths from drug self-intoxication, has surpassed diabetes as the seventh leading cause of death in the United States, prompting researchers to call for a new unified approach to SIM prevention.
Senior Citizens need to have comprehensive medical evaluations that are readily available to emergency providers. Electronic Medical Recording is ideal for having much needed information at the proper person's finger tips. The hesitancy of primary care physicians to employ EMR/EHR systems places a heavy burden on emergency departments in the United States. Senior citizens often have special needs that are not readily known by first responders and in a crisis situations, the care provided is based on standard of care and not special needs. Innovative alternatives to the current data taking, storage and retrieval process.
Diabetes & Texas Medicaid Savings 11 01thoenner
Diabetes affects nearly 24 million people in the United States, an increase of more than 3 million in just two years. The Diabetes epidemic cost the U.S. economy more than $200 billion each year in medical expenses and lost productivity. This presentation outlines the challenges and proposes practical proven solutions aimed at improving outcomes while reducing the cost of treating Medicaid eligible Texans with diabetes.
SBIRT and SAMHSA's 8 Strategic Initiativessideponytail
Slides from a webinar held by the National SBIRT ATTC. Video is on TheIRETAChannel on Youtube: http://www.youtube.com/watch?v=f6NrKuGlGRs&feature=share&list=PLiML4AFpuB72LBaPShcu2yQv_WpsGY9a9
Empowering Healthcare Leaders: The Business Case for Language Access_10.3.14Douglas Green
Empowering Healthcare Leaders: The Business Case for Language Access provides a framework for calculating total potential encounters with limited English patients, the economic benefit and cost of not providing language access and a frame work to align the economic benefits with organizational goals under the Affordable Care Act.
Addiction Medicine: Closing the Gap between Science and PracticeCenter on Addiction
These slides accompany CASAColumbia's report, Addiction Medicine: Closing the Gap between Science and Practice, published in June 2012, which found that, despite the prevalence of addiction, the enormity of its consequences, the availability of effective solutions and the evidence that addiction is a disease, both screening and early intervention for risky substance use are rare, and only about 1 in 10 people with addiction involving alcohol or drugs other than nicotine receive any form of treatment.
2014 National Healthcare Quality and Disparities Report Chartbook on Care Aff...Ernest Moy
This Care Affordability chartbook is part of a family of documents and tools that support the National Healthcare Quality and Disparities Report (QDR). The QDR includes annual reports to Congress mandated in the Healthcare Research and Quality Act of 1999 (P.L. 106-129). This chartbook includes a summary of trends across measures of care affordability from the QDR and figures illustrating select measures of care affordability.
This essay is prepared with an aim to investigate into the difficulties arises while dealing
with alcoholic patients in primary care in Europe. In this context, the researcher will evaluate the
issues concerned with doctors in tackling the psychological character of alcoholic patients.
Moreover, the discussion will provide how doctors motivate such patient to recover from their
lethal conditions. In spite of declining in the wine-producing nations, Europe remains the
province on the globe with largest production as well as consumption of alcoholic beverages
along with commensurately more levels of harm related to alcohol. In the survey of North
America it was found that over 4.5% of women and 23% of men are involved in the alcohol use
or dependence throughout their lifetime. The country is about the middle of the worldwide
league of intoxicating consumption. Thus, in all European Union’s member states the alcoholic
harms are considered as a major public health problem. The use of alcohol and its harm are
increasing sharply in the some recently independent regions of Eastern Europe.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
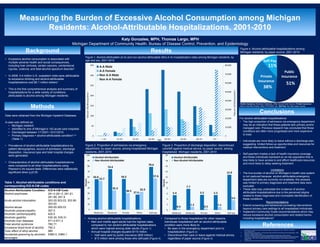
1. Measuring the Burden of Excessive Alcohol Consumption among Michigan
Residents: Alcohol-Attributable Hospitalizations, 2001-2010
Background
Conclusions
Katy Gonzales, MPH, Thomas Largo, MPH
Michigan Department of Community Health, Bureau of Disease Control, Prevention, and Epidemiology
Methods
Results
References
• Excessive alcohol consumption is associated with
multiple adverse health and social consequences,
including liver cirrhosis, certain cancers, unintentional
injuries, violence, and fetal alcohol spectrum disorder1.
• In 2006, 4.4 million U.S. outpatient visits were attributable
to excessive drinking and alcohol-attributable
hospitalizations cost $5.1 million dollars1.
• This is the first comprehensive analysis and summary of
hospitalizations for a wide variety of conditions
attributable to alcohol among Michigan residents.
Data were obtained from the Michigan Inpatient Database.
A case was defined as:
• Michigan resident
• Admitted to one of Michigan’s 142 acute care hospitals
• Discharged between 1/1/2001-12/31/2010
• Primary diagnosis = alcohol-attributable condition2,3,4
(Table 1)
• Prevalence of alcohol-attributable hospitalizations by
patient demographics, source of admission, discharge
disposition, insurance type and total hospital charges
were generated.
• Characteristics of alcohol-attributable hospitalizations
were compared to all other hospitalizations using
Pearson’s chi-square tests. Differences were statistically
significant when p<0.05.
1. Bouchery et. Al. Economic Costs of Excessive Alcohol Consumption in the U.S., 2006. Am J Prev Med
2011;41(5):516–524
2. National Institute on Drug Abuse. The Economic Costs of Alcohol and Drug Abuse in the United States - 1992.
Appendix A: Health Disorder Codes
3. Centers for Disease Control and Prevention; Alcohol-Related Disease Impact (ARDI) Software.
4. Chen CM, Y, H. (2008) Trends in Alcohol-Related Morbidity Among Short-Stay Community Hospital Discharges,
United States, 1979 - 2006. Surveillance Report #84. National Institute on AlcoholAbuse and Alcoholism,
Arlington, VA.
5. The Guide to Community Preventive Services. http://www.thecommunityguide.org/alcohol/index.html
For alcohol-attributable hospitalizations:
• The high proportion of admission via emergency department
may be an indication that these patients lack primary and/or
managed care. Previous research has concluded that these
conditions are often more progressed and more expensive
to treat.
• Individuals are more likely to leave without a discharge plan,
suggesting limited follow-up opportunities and resources for
medical interventions and treatment.
• Self-payment implies a lack of health insurance coverage
and these individuals represent an at-risk population that is
less likely to have access to and afford healthcare resources
and more likely to delay seeking treatment.
Limitations
• The true burden of alcohol on Michigan’s health care system
is not captured because alcohol-attributable emergency
department data are currently not available; this analysis
was limited to primary diagnoses and treatment data were
excluded.
• These data may understate the incidence of alcohol-
attributable hospitalizations due to the perceived stigma
related to these diagnoses and incomplete identification of
these conditions.
Recommendations
• Extend screening and behavioral counseling interventions
beyond primary care settings to all hospitalized individuals.
• Implement Community Guide recommendations which may
reduce excessive alcohol consumption and related harms,
including hospitalizations5.
Alcohol-Attributable Condition ICD-9-CM Code
Alcohol psychoses 291.0-291.5, 291.81,
291.89, 291.9
Acute alcohol intoxication 303.00-303.03, 303.90-
303.93
Alcohol abuse 305.00-305.03
Alcoholic polyneuropathy 357.5
Alcoholic cardiomyopathy 425.5
Alcoholic gastritis 535.30, 535.31
Alcoholic liver diseases 571.0-571.3
Fetal alcohol syndrome 760.71
Excessive blood level of alcohol 790.3
Toxic effect of ethyl alcohol 980
Accidental poisoning by alcoholic
beverages
E860.0, E860.1
Table 1. Alcohol-attributable conditions and
corresponding ICD-9-CM codes
Figure 2. Proportion of admissions via emergency
department, by payer source, among hospitalized Michigan
residents, 2001-2010
Figure 3. Proportion of discharge disposition: discontinued
care/left against medical advice, by payer source, among
hospitalized Michigan residents, 2001-2010
Figure 4. Alcohol-attributable hospitalizations among
Michigan residents, by payer source, 2001-2010
• Among alcohol-attributable hospitalizations:
• Men and middle aged adults had the highest rates,
compared to non alcohol-attributable hospitalizations
which were highest among older adults (Figure 1)
• Annual hospital charges equaled $115 million
• Half were paid by public insurance ($59 million)
• $13 million were among those who self-paid (Figure 4)
• Compared to those hospitalized for other reasons,
individuals hospitalized with an alcohol-attributable
condition were more likely to:
• Be seen in the emergency department prior to
hospitalization (Figure 2)
• Discontinue their care or leave against medical advice,
regardless of payer source (Figure 3)
Figure 1. Alcohol-attributable (A-A) and non alcohol-attributable (Non A-A) hospitalization rates among Michigan residents, by
age and sex, 2001-2010
51%
38%
11%
Self‐Pay
Private
Insurance
Public
Insurance
Public Insurance: Medicaid, Medicare, Other Government Source. Private Insurance:
Blue Cross Blue Shield, Other PPO/HMO, etc. Self-Pay: No other payer source.
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
0
50
100
150
200
250
300
350
< 14 15‐24 25‐34 35‐44 45‐54 55‐64 65‐74 75+
Rate per 100,000 population
Rate per 100,000 population
Age
A‐A Male
A‐A Female
Non A‐A Male
Non A‐A Female
5.4
7.7
5.5 5.5
12.9
0.4
1.2
0.5
1.1
3.6
0
2
4
6
8
10
12
14
16
18
20
Medicare Medicaid Private Other Self‐pay
Percent
Alcohol‐Attributable
Non Alcohol‐Attributable
56.0
74.4
56.5
27.6
78.6
52.7
35.3
30.5 32.9
57.6
0
10
20
30
40
50
60
70
80
90
100
Medicare Medicaid Private Other Self‐pay
Percent
Alcohol‐Attributable
Non Alcohol‐Attributable