
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Peptic ulcer
Similar to Peptic ulcer (20)
Recently uploaded
Recently uploaded (20)
Peptic ulcer
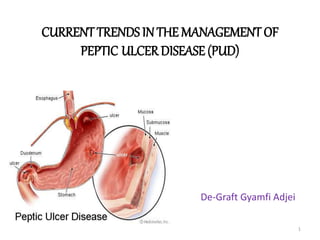
- 1. CURRENTTRENDS IN THE MANAGEMENT OF PEPTIC ULCERDISEASE (PUD) De-Graft Gyamfi Adjei 1
- 2. OUTLINE • INTRODUCTION – DEFINITION – HISTORY • EPIDEMIOLOGY • ETIOLOGY • ANATOMY • PATHOPHISIOLOGY • CLINICAL PRESENTATIONS • INVESTIGATIONS • MANAGEMENT • ACKNOWLEDGENT • REFERENCES 2
- 3. INTRODUCTION • Peptic ulcer refers to a break in the lining of the stomach, first part of the small intestine or occasionally the lower oesophagus. 3
- 4. CLASIFICATION OF PEPTIC ULCER DISEASE • The major forms of PUD are: – Gastric Ulcer – Duodenal Ulcer • Gastric Ulcer: ulcers that occur in the stomach • Duodenal Ulcer: ulcers that occur in the upper area of the small intestine 4
- 5. SYMPTOMS OF DUODENAL ULCERS • Localized pain(pin point), restricted to mid-epigastrum • Nocturnal pain • Relieved by food and antacids • Pain may radiate to costal margins of the back or the right shoulder • Weight gain (probably due to ↑ urge to eat to relieve pain) 5
- 6. SYMPTOMS OF GASTRIC ULCERS • Pain is more diffuse – over a wide area of mid epigastric region • Rarely produces nocturnal pain • Pain precipitated by food • Pain may be referred to the left subcostal region • Weight loss common with GU 6
- 7. HISTORY • EARLY 20TH CENTURY: – Ulcers were believed to be caused by stress an dietary factors. – Later gastric acid was blamed for peptic ulcer disease 7
- 8. …HISTORY • 1982 – first identified the link between Helicobacter pylori and ulcers. • 1994 – NIHCDC concluded that there Is a strong link between H. pylori and ulcer dxs – Pxs be treated with antibiotics 8
- 9. …HISTORY • 1996 – The FDA approves the first antibiotic for treatment of ulcer disease • 1997 – The CDC launches campaign to inform healthcare providers and consumers about the link between H. pylori and ulcers 9
- 10. EPIDEMIOLOGY • In the US, PUD affects 4.5million people annually • Approximately 10% of the US population has evidence of duodenal ulcer at some time, • Of those infected with H. pylori, the lifetime prevalence is approx. 20% • Only about 10% of young persons have H. pylori infection 10
- 11. EPIDEMIOLOGY • Overall, the incidence of Duodenal ulcer has been decreasing over the past 3-4 decades • The prevalence of PUD has shifted from predominance in males to similar occurences in males and females • In May 2014, WHO established that in Ghana, the death rate due to PUD was 9.55 per 100,000 persons 11
- 12. EPIDEMIOLOGY(KBTH) • Patience attendance at OPD – 2013- 13744 persons – 2014- 13051 persons • Out of the above population, PUD cases were 587(4.2%) in 2013 and 1177(9.01%) in 2014 • Females represented 55-58% of the population recorded • <5% had surgery 12
- 13. EPIDEMIOLOGY(KBTH) • At the endoscopy unit, 1144(36.0%) were confirmed to have PUD in 2013 • PUD was ranked one of the top 10 causes of admission for three consecutive years • PUD was ranked the 9th major cause of admission(in males) and 10th in females at the polyclinic 13
- 14. EPIDEMIOLOGY 0 20 40 60 80 100 120 140 2012 2013 2014 F R E Q U E N C Y YEARS TOP TEN CAUSES OF ADMISSION AT GENERAL SURGERY 14
- 15. ETIOLOGY • The 2 most common risk factors for PUD are: – Helicobacter pylori – Non steroidal anti- inflammatory drugs • Other uncommon risk factors include: – Lifestyle factors(e.g ageing, smoking, alcohol intake) – Severe physiologic stress – Hypersecretory states – Genetic factors 15
- 17. Helicobacter pylori • H. pylori is a Gram-negative, spiral & microaerophyllic bacterium with multiple flagella at one end • Adheres to gastric epithelial lining. • Produces various enzymes - urease, haemolysins, fusidase, neuraminidase. • About 2/3 of world population infected , with an estimated prevalence of 80-90 % in the developing world 17
- 18. Helicobacter pylori • Infected persons have up to 6-fold increased risk of developing gastric cancers • Most likely spread from person to person through faecal-oral and oral-oral routes. 18
- 19. Pathogenesis of H. pylori infection • The Flagella make it motile, allowing it to live deep beneath the mucus layer • It uses an adhesin molecule to bind to epithelial cells Where the pH there is close to neutral 19
- 20. 2. Etiology -Non-Steroidal Anti-inflammatory Drugs (NSAIDS) • Symptomatic GI ulceration occurs in 2% - 4% of patients treated with NSAIDs for 1 year • The effects of aspirin & NSAIDs on the gastric mucosa ranges from mucosal hemorrhages to erosions & acute ulcers 20
- 21. NSAIDS • Inhibit the production of prostaglandins resulting in: – 1. Decrease mucus & HCO3 production – 2. Decrease mucosal blood flow – 3. Reduce cell renewal • HCl aggravates NSAID- induced mucosal injuries by – Converting superficial injury to deeper mucosal necrosis, – Interfering with haemostasis & platelet aggregation – Impairing ulcer healing 21
- 22. Types of NSAID & Risk of Ulcer 22 Risk Group Drug Low Ibuprofen Medium Naproxen Diclofenac Indomethacin High Piroxicam,Ketoprofen Azapropazone
- 23. PATHOPHYSIOLOGY • The upper G.I system consists of – Oesophagus – Stomach – Duodenum • Stomach – Cardia: secretion of mucous – Body: • parietal cells • Chief cells – Antrum: • G cells • D cells 23
- 24. PATHOPHYSIOLOGY • Gastric Secretions (About 2.5L HCL daily) • smooth muscle – churning • sub-mucosa – veins and arteries that carries blood to the liver 24
- 25. PATHPHYSIOLOGY • The gastroduodenal mucosal integrity is determined by adequate balance between protective(defensive) and damaging(aggressive) factors • When the aggressive factors increase or the defensive factors decrease, mucosal damage will result leading to ulcerations 25
- 26. PATHOPHYSIOLOGY • DEFENSIVE FACTORS – Bicarbonate – Mucus layer – Mucosal blood flow – Prostaglandins – Rapid epithelial renewal • AGGRESSIVE FACTORS – Helicobacter pylori – HCl – NSAIDs – Stress – Smoking& alcohol – Ageing 26
- 28. PATHOPHYSIOLOGY • Two major variants in peptic ulcers are commonly encountered in the clinical practice: 1. Duodenal Ulcer (DU) 2. Gastric Ulcer (GU) • DU: increased acid load to the duodenum due to: • Increased parietal cell mass • Increased gastrin secretion (e.g. Zollinger-Ellison syndrome, alcohol & spicy food) • H. pylori damaging somatostatin-producing cells • Increased gastric emptying rate • HCO3 secretion is decreased in the duodenum by H. pylori inflammation • Increased vagal nerve stimulation 28
- 29. PATHOPHYSIOLOGY GU results from the break down of gastric mucosa: 1) The local epithelial damage due to cytokines released by H. pylori 2) Pyloric sphincter dysfunction or obstruction 3) Reflux of bile salts into the stomach 4) Nicotine- delaying ulcer healing 29
- 30. Pathogenesis of H. pylori infection • Effects of H. pylori on gastric Hormones 30 - ↓ Somatostatin production from antral D-cells due to antral gastritis - Low somatostatin will ↑Gastrin release from G-cell hypergastrinemia - This will stimulate acid production by the parietal cells leading to further duodenal ulceration. This effect is exaggerated among smokers!
- 31. DIAGNOSIS • Involves 3 Criteria – Patient history taking Risk Factors Symptoms – Clinical Signs epigastric tenderness GI bleeding – Investigations • Endoscopy for ulcer detection • H. pylori Detection 31
- 32. DIAGNOSIS OF H. pylori • Non-invasive – C13 or C14 Urea Breath Test – Stool antigen test – H. pylori IgG titer (serology) • Invasive – Gastric mucosal biopsy with histology – Rapid Urease test (CLO test) 32
- 33. DIAGNOSIS OF H. pylori Non-invasive 1. C13 or C14 Urea Breath Test 33 The best test for the detection of an active infection
- 34. DIAGNOSIS Non-invasive Serology for H pylori Serum Antibodies (IgG) to H pylori (Not for active infection) Fecal antigen testing (Test for active HP). Invasive Upper GI endoscopy Highly sensitive test Patient needs sedation 34
- 35. Endoscopy (Invasive) Detects the site and the size of the ulcer, even small and superficial ulcer can be detected Detect source of bleeding Biopsies can be taken for rapid urease test, histopathology & culture 35
- 36. Invasive (endoscopy) Rapid urease test ( RUT) Considered the endoscopic diagnostic test of choice Gastric biopsy specimens are placed in the rapid urease test kit. If H pylori are present, bacterial urease converts urea to ammonia, which changes pH and produces a COLOR change 36
- 37. Duodenal Ulcer on Endoscopy 37 Normal duodenal bulb Duodenal Ulcer
- 38. Gastric Ulcer on Endoscopy 38 Chronic Gastric Ulcers
- 40. PUD COMPLICATIONS • GI bleeding • Perforation • Gastric /duodenal obstruction(presents with projectile vomiting, pyloric stenosis) • Haemorrhage –may lead to Chronic anemia • Recurrence • Malignancy- gastric ulcers 40 Bleeding DU Perforated GU Duodenal stricture
- 41. PUD COMPLICATIONS 41 OBSTRUCTION – PYLORIC STENOSIS
- 42. PUD and CANCER • Vacuolating cytotoxins(vac A) – Pore-forming proteins – Permeability – Suppresses immunity • Cytotoxin associated gene (cag A) – Oncogenic proteins – Changes morphology – Apoptosis 42
- 43. INTERVENTIONS • Surgical interventions may be required in certain cases – Malignant ulcers – Pyloric stenosis – Chronic ulcerations – Uncontrolled bleeding – perforations • 3 main surgical procedures – Vagotomy – Antrectomy – Pyloroplasty 43
- 44. MANAGEMENT OF PEPTIC ULCER DISEASE 44
- 45. NON PHARMACOLOGICAL TREATMENT • Avoid smoking/smoke cessation • Avoid foods that aggravate the pain • Allay anxiety and stress; reduced if possible • Regular small meals • Moderation of coffee and tea • Avoid late night snacks as they stimulate nocturnal gastric acid secretion • Avoid alcohol • Have enough rest • Avoid NSAID’s when necessary 45
- 46. GOALS OF TREATMENT • Pharmacological treatment – To relieve pain and reduce gastric acid secretions – To promote healing of the ulcer – To eradicate H. pylori if present – To prevent recurrence of ulcer – To avoid complications 46
- 47. PEPTIC ULCER DRUGS • Proton pump inhibitors (PPI) • H2 – receptor antagonist • Prostaglandin analogues • Sucralfate • Antacids • BISMUTH CHELATES(no longer used ; neurotoxic) • Selective anti-muscaranics (Pirenzepine) 47
- 48. PROTON PUMP INHIBITORS- PPI’s • PPI’s are weak bases and hence need enteric coating to protect it from the acidic state of the stomach • PPI’s bind irreversibly to the proton pump, hence have more sustained duration of acid inhibition • Should be taken 30minutes before meals • PPI’s should not be given before an endoscopy as they may mask serious underlying pathology 48
- 49. EXAMPLES OF PPI’S • Omeprazole/ Esomeprazole • Lansoprazole • Pantoprazole 49
- 50. PPI’s contd Mechanism of action: – Inhibits the production of gastric acid by blocking the hydrogen-potassium adenosine triphosphate enzyme system (h+k+=atpase) of gastric parietal cells in the gastric mucosa – Thus the exchange of hydrogen and potassium across the membrane to maintain gastric acidity is inhibited 50
- 51. PPI’s • Adverse effects: – Usually mild and reversible – Diarrheoa – Headache – Nausea – Abdominal pain – Constipation and dizziness • Prolonged use of PPI’s is associated with hypomagnesemia 51
- 52. Pharmacokinetics of PPI’s Characteristic Omeprazole Lansoprazole Rabeprazole Pantoprazole Esomeprazole Bioavailability( %) 30-40 80-85 52 77 64-89 Time to peak [plasma] (hrs) 0.5-3.5 1.7 2.0-5.0 1.1-3.1 1-2 Plasma elimination t1/2 (hrs) 0.5-1 1.3-1.7 1.0-2.0 1.0-1.9 1.3 Protein binding(%) 95 97 96 98 97 Urinary excretion of oral dose(%) 77 14-23 30-35 71-80 80
- 53. H2 RECEPTOR ANTAGONIST- H2RA’s • Mechanism of action – By blocking histamine type two receptors in gastric parietal cells – Thus, preventing acid secretion to reduce gastric output • H2 receptor antagonists in combination with PPI at bedtime may enhance gastric PH control at night 53
- 54. EXAMPLES OF H2RA’s • Ranitidine • Cimetidine • Fomatidine • Nizadine 54
- 55. H2RA’s • Effectively heal ulcers when NSAID therapy is stopped • main role of H2RA is the empirical management of dyspepsia symptoms 55
- 56. ADVERSE EFECTS OF H2RA’s • Diarrhea • Headache • Dizziness • Rash • Tiredness • Gynaecomastia and impotence occur occasionally with cimetidine 56
- 57. Comparison of H2-receptor antagonists. Variable Cimetidine. Ranitidine. Nizatidine. Famotidine. Brand name Tagamet Zantac Axid Pepcid Rel. potency 1 4-10 4-10 20-50 Dose to heal DU(mg) 300 qid 400 bd 800 nocte 150 bd 300 nocte 150 bd 300 nocte 40 nocte Maintenance dose (mg) 400 nocte 150 nocte 150 nocte 20 nocte Dose to heal GU (mg) 300 qid 400 bd 800 nocte 150 bd N/A N/A ABSORPTION Bioavailability (%) 30-80 (60) 30-88 (50) 75-100 (98) 37-45 (43) Time to peak [serum] (hr) 1-2 1-3 1-3 1-3.5 VOD (L/kg b.w) 0.8-1.2 1.2-1.9 1.2-1.6 1.1-1.4
- 58. PROSTAGLANDIN ANALOGUES • Mechanism of action: – Has antisecretory and protective properties promoting peptic ulcer healing – Can be used as prophylaxis against NSAID induced ulcers • Example: Misoprostol ( Cytotec) 58
- 59. SIDE EFFECTS • Diarrhea (it may be severe and require withdrawal) • Nausea &vomiting • Dyspepsia • Abnormal vagina bleeding with menorrhagia • Flatulence • Abortifaecient 59
- 60. SUCRALFATE • Aluminium salt of sucrose octasulphate • Weak antacid • Has mucosal protective effects by stimulating bicarbonates and mucos secretion and stimulation of mucosal prostanoids • Effective in the treatment of NSAID induced ulcers if NSAID’s are stopped(2g daily) • Main side effect is constipation 60
- 61. ANTACIDS • Acts by neutralizing gastric acid • However only effective for a short period • Alginates are added to antacids to relieve reflux symptoms • Antacids are best given when symptoms occur or are expected 61
- 62. ANTACIDS • Side effects of antacid are considered in choosing type of antacid • Aluminium salt antacids may cause constipation • While magnesium salts may cause diarrhea • Hence a combination of these are preferred to produce neutral effect on intestinal transit • Calcium containing antacid may have an effect of rebound acid secretion as calcium stimulates acid secretion – Also regular intake may cause hypercalcemia 62
- 63. ANTACIDS • Antacids containing sodium bicarbonates should not be given to patients on restricted salt diet • Magnesium trisilicate has very high sodium bicarbonate content • Liquid antacids are usually preferred over tablets – Antacid Dosing: 10-15mL 8 or 6 hourly; of liquid Mg-Al antacids promote ulcer healing, but less than antisecretary drugs 63
- 64. ADVERSE EFFECTS OF ANTACIDS • Constipation (Aluminium) • Diarrhoea (Magnesium) • Flatulence(Carbonates & bicarbonates) • Nausea & vomiting 64
- 65. EXAMPLES OF ANTACIDS • Magnesium sulfate • Aluminium salts • Calcium carbonate • Sodium bicarbonate 65
- 66. Neutralizing capacity of some commonly used antacid atacid Active components Neutralising capacity (mEq) Ducon Al(oh)3 Mg(oh)2 caco3 7.04 Maalox Al(oh)3 Mg(oh)2 2.58 Maalox plus Al(oh)3 Mg(oh)2 simethicone 2.30 Nugel AL(OH)3 Mg(OH)2 MAGNESIUM TRISILLICATE ALGINATE SIMETHICONE aludrox Al(oh)3 Mg(oh)2 2.81 66
- 67. Management- H. pylori eradication • Most patients with DU are infected with H. pylori • Eradicate with 7 day course of PPI plus combination of antibiotics classes of antibiotics used include: – Macrolide (clarithromycin) – Penicillin(amoxycillin) – Metronidazole • For initial therapy against H. pylori a 7-10 day triple therapy comprising of a PPI or H2ra, Clarithromycin, and either amoxicillin or metronidazole • For a quadruple therapy, bismuth chelate is added. • These regimen eradicate h. pylori 85% of cases • Dual therapy of PPI and one antibiotic can be used, but produces low rates of eradication • PPI regimen is continued for 4-8 weeks to ensure wound healing 67
- 68. Amoxycillin • Active against H. pylori • Shown to be 90% active against H. pylori • Should not be given to patients with true penicillin allergy • Erythematous rash • Maculopapular rash • GI adverse effects do not constitute allergy (nausea, vomiting, diarrhoea) • Uticarial rash does not constitue true penicillin allergy 68
- 69. Clarithromycin • Very active against h. pylori • Generally well tolerated • May cause GI adverse effects such as: – Nausea – Diarrhoea – Vomiting • Not given to pregnant and lactating women, excreted in milk 69
- 70. Metronidazole • Active against gram negative bacteria including h. pylori • Causes disulfiram-like reactions with alcohol • Side effect: • Metallic taste in mouth • GI irritations including nausea and vomiting • Metronidazole is not the first line antibiotic in h. pylori eradication • But it can be given when there’s treatment failure, symptoms do not resolve. • Tinidazole can be give in place of Metronidazole. 70
- 71. Current trends in management Of peptic ulcer disease 71
- 72. Overview of treatment • Give initial treatment • Test for H. pylori • Endoscopy and H.pylori retesting • Stop NSAID use if possible • Ongoing care if symptoms recur or continues 72 NICE guidelines (2015)
- 73. Initial treatment – Offer H. pylori eradication therapy to people who have tested positive for H. pylori and who have peptic ulcer disease. – For people using NSAIDs with diagnosed peptic ulcer, stop the use of NSAIDs where possible. – Offer full-dose PPI or H2RA therapy for 8 weeks and, if H. pylori is present, subsequently offer eradication therapy. – Offer full dose PPI or H2ra for4-8 weeks for people who have tested negative for H. pylori and are not on NSAID’s 73
- 74. 74
- 75. ENDOSCOPY & H. PYLORI RETESTING • Repeat endoscopy and H. pylori retesting for patient 6-8 weeks after treatment • This depends on the size of the lesion • Carbon 14 breath test may be insufficient at this stage 75
- 76. NSAID USE • Discuss potential of nsaid treatment for people who have to take NSAID’s after the ulcer is healed • Review the need for NSAID use regularly, at least every 6 months • Consider dose reduction or substituting with paracetamol • Or use an alternative or low dose ibuprofen • If NSAID continuation is very necessary, consider cox 2 selective NSAIDs 76
- 77. UHEALED ULCER/ CONTINUED SYMPTOMS/ RECURRENCE • In people with an unhealed ulcer, rule out – non-adherence, – malignancy, – failure to detect H. pylori, – inadvertent NSAID use or other ulcer-inducing medication – and rare causes such as Zollinger–Ellison syndrome or Crohn's disease. • If symptoms recur after initial treatment, offer a PPI to be taken at the lowest dose possible to control symptoms. • Discuss using the treatment on an 'as-needed' basis with people to manage their own symptoms. 77
- 78. Current drug regimen- H. pylori eradication PPI ANTIBIOTIC amoxicillin clarithromycin metronidazole Esomeprazole 20mg 12hrly 1g 12hrly 500mg 12hrly ------------ ----------- 500mg 12hrly 400mg 12hrly Omeprazole 20mg 12hrly 1g 12hrly 500mg 12hrly ------------ 500mg 8hrly -------------- 400mg 8hrly -------- 500mg 12hrly 400mg 12hrly Rabeprazole 20mg 12hrly 1g 12hrly 500mg 12hrly --------- ----------- 500mg 12hrly 400mg 12hrly 78
- 79. CURRENT DRUG REGIMEN- NSAID INDUCED ULCERS • Esomeprazole, oral: – Adults:-20 mg daily for 4 weeks. Repeat course if ulcer is not fully healed. • Or Omeprazole, oral, – Adults:20 mg daily for 4 weeks. Repeat course if ulcer is not fully healed. • Or Rabeprazole, oral, – Adults:20 mg daily for 4 weeks. Repeat course if ulcer is not fully healed. 79
- 80. CURRENT DRUG REGIMEN- BLEEDING PEPTIC ULCER • · Esomeprazole, IV, – Adults:40 mg daily • Or Omeprazole, IV, – Adults:40 mg 12 hourly for up to 5 days 80
- 81. PATIENT EDUCATION • Seek pharmacist advice when purchasing OTC analgesics • Patients with risk of peptic ulceration should be advised to avoid otc aspirin and NSAIDs • Taking aspirin and NSAIDs with or after food may decrease risk of dyspepsia • Patient should be aware of optimum time for administration of PPI, dose duration therapy • Misoprostol should not be used in pregnant women and women of child bearing age • Patients need to know the importance of adherence to eradication therapy for successful treatment, to prevent resistance 81
- 82. ROLE OF THE PHARMACIST… • Pharmaceutical care for peptic ulcer patients – Monitoring treatment – Efficacy of treatment: (the signs and symptoms and investigations are looked) – the toxicity of the medicines: (relies on harmful side effects). – Counselling • if patients are adequately counselled on their disease, aims of therapy, life style modification and advice on managing side effects effective concordance can be obtained. 82
- 83. ROLE OF THE PHARMACIST • General public (patient) Education and Counseling on; – Potentially harmful agents, including: • NSAIDs • Aspirin • Alcohol • Tobacco • Caffeine – Stress Reduction 83
- 84. CONCLUSION • An understanding of how peptic ulcer occurs, in concept with a good knowledge of potent acid suppressing drugs as well as the implication of H. pylori in PUDs have changed the face of ulcer therapy providing hope for better prognosis over time. 84
- 85. REFERENCES • Annual Report,2013, Korle Bu Teaching Hospital, pp 22,111-112 • British National Formulary (BNF) 68th edition • Hatakeyama, M et al (2014). H.pylori cagA and gastric cancer: a paradigm for hit and run carcinogenesis • Etc…… 85
- 86. THANK YOU 86
Editor's Notes
- The trtment focuses on bed rest hospitalization and prescription of special bland foods. Antacids an medications that block acid secretion became the standard of therapy Despite treatment, theres a high recurrence of ulcers
- Australian physicians Robin Warren and Barry Marshall National Institute of Health Consensus Development Conference they recommended that ulcer pts with h. pylori infection shud b treated with antibiotics.
- CENTER FOR DISEASE CONTROL AND PREVENTION
- Severe physiologic stress as a result of burns trauma surgery and severe medical ilness Lifestyle factors include smoking alcohol diet More than 20% of pts have a family history of DU compared to 5-10% in the control groups DU and blood type O is a weak association that has been observed but the reason is unclear Egs of hypersecretory states are gastrinoma or multiple endocrine neoplasia type 1