
Downloaded 30 times

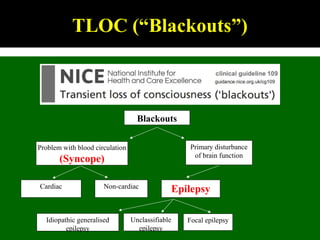
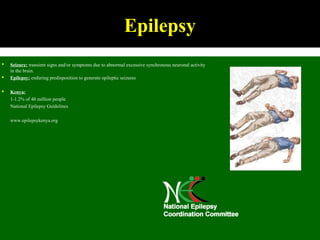
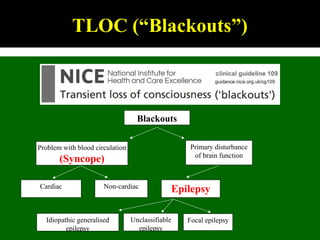
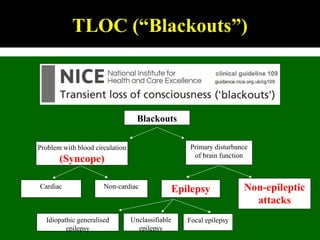
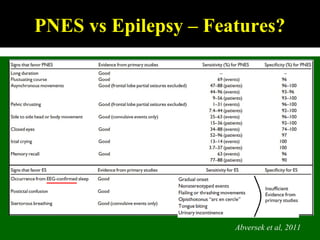
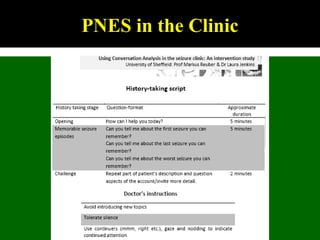
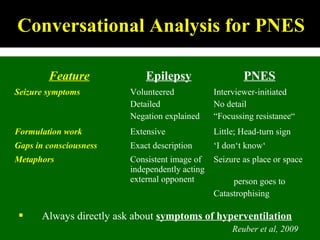
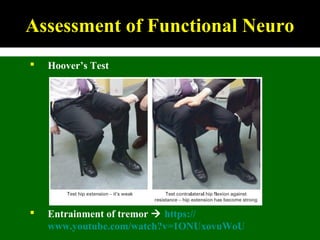
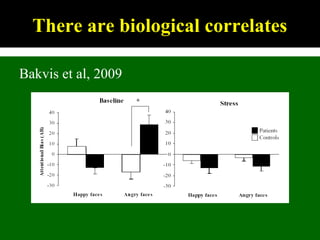
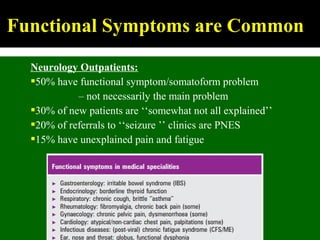
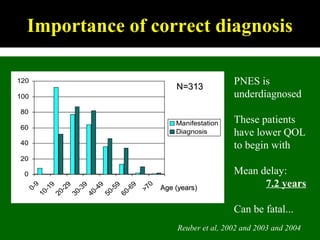
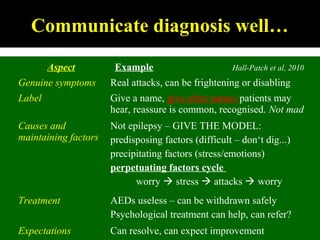
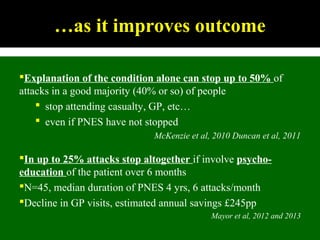
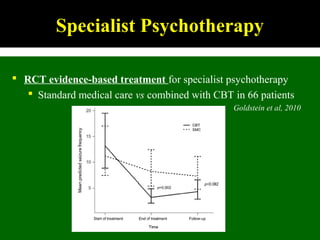
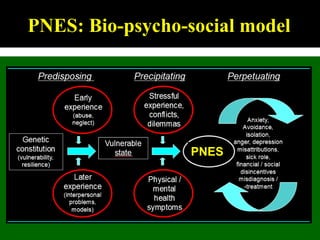

This document outlines Dilraj S. Sokhi's presentation on neurological manifestations of psychological problems. It discusses transient loss of consciousness (TLOC), psychogenic non-epileptic seizures (PNES), medically unexplained symptoms (MUS), and cognitive behavioral therapy (CBT). The presentation describes the differences between epileptic and non-epileptic seizures, predisposing and precipitating factors for PNES, diagnostic tools like video EEG, and the importance of correctly diagnosing and explaining PNES to patients. It emphasizes treating the whole patient using a biopsychosocial model and mentions the recognition and management of PNES may be important in Kenya given psychological comorbidities in the population.


























































