

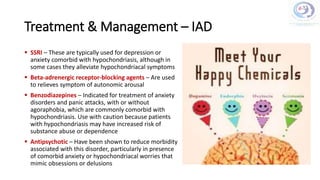


The document discusses illness anxiety disorder (IAD), outlining a case study of a 45-year-old male engineer who is preoccupied with having cancer despite inconclusive medical evaluations. It highlights the challenges in diagnosing and treating IAD, emphasizing its psychological complexities and the importance of a collaborative treatment approach involving various healthcare professionals. The document also reviews epidemiology, symptoms, causes, and several treatment strategies, including cognitive-behavioral therapy and pharmacotherapy.














![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)




















































