Downloaded 31 times
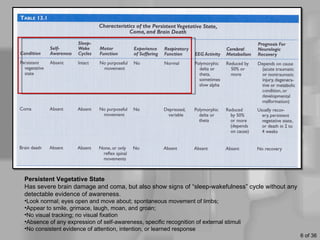

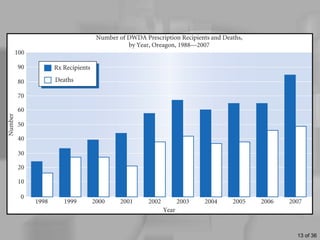

This document discusses definitions of death, ethical issues surrounding end of life care, and personal aspects of thinking about death. It defines clinical death, whole brain death, and persistent vegetative state from a legal and medical perspective. Ethical issues discussed include euthanasia, assisted suicide laws, advance directives, do not resuscitate orders, and the high costs of life-sustaining care. Case studies on Nancy Cruzan and Terri Schiavo are provided. Developmental views of how people think about death across the lifespan and Kübler-Ross's five stages of grief are also summarized.























































































