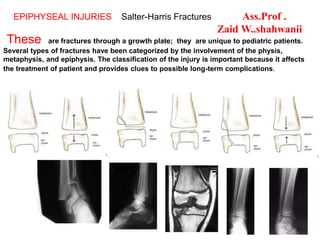
1. These are fractures through a growth plate; they are unique to pediatric patients.
Several types of fractures have been categorized by the involvement of the physis,
metaphysis, and epiphysis. The classification of the injury is important because it affects
the treatment of patient and provides clues to possible long-term complications.
EPIPHYSEAL INJURIES Salter-Harris Fractures Ass.Prof .
Zaid W..shahwanii
2. THE INJURIES OF THE PHYSIS
Special problems to children. They may cause growth
abnormalities.
The children bones grow on their ends through an epiphysial
plate (also called physis) that lay down new bone in both
directions towards the joint and that part is called epiphysis,
and toward the shaft and that part is called metaphysis. The
shaft itself is called diaphysis.
The epiphysial plate appears radiolucent on x ray because
they are mainly of cartilage. This growing plate will stop
growing, gradually ossifies and disappears around the time of
skeletal maturity.
Each plate disappears at different time during life. Injuries
and fractures at the region of epiphyseal plate carry the bad
and serious complications of disturbing or stopping bone
growth of all or part of the epiphysial plate giving rise to
lateral shortness or deformities of the involved limb or joint.
5. The classification of Salter-Harris
fractures is used to describe the
extent & site of the epiphyseal
injuries
Type I
A type 1 fracture is a transverse
fracture Through the hypertrophic
zone of the physis.
In this injury, the width of the physis
is
increased.or there will be a transverse
separation of the physis from the
metaphysis ..
The growing zone of the physis usually
is not injured, and growth
disturbance is uncommon
.
On clinical examination, the child
has point tenderness at the which is
suggestive of a type I fracture
epiphyseal plate,
6. Salter-Harris_Epiphyseal injuries
II
Type
A type II fracture is a
fracture through the
physis and the
metaphysis, but the
epiphysis is not involved
in the injury
.
These fractures may
cause minimal
shortening; however, the
injuries rarely result in
functional limitations
Type II is the most
common type of
Salter-Harris fracture
7. Type III
A type III fracture is a fracture
through the physis and the
epiphysis. This fracture passes
through the hypertrophic layer of
the physis and extends to split the
epiphysis, inevitably damaging
the reproductive layer of the
physis
.
This type of fracture is prone to
chronic disability because by
crossing the physis, the
fracture extends into the articular
surface of the bone
.
However, type III fractures rarely
result in significant deformity;
therefore, they have a relatively
favorable prognosis ,,,,,The
treatment for this fracture is often
surgical
9. Type IV
fracture involves all 3
elements of the bone: The
fracture passes through the
epiphysis, physis, and
metaphysis
.
A type IV fracture is an
intra-articular fracture;
thus, it can result in
chronic disability
By interfering with the
growing layer of cartilage
cells, these fractures can
cause premature focal
fusion of the involved bone.
Therefore, these injuries
can cause deformity of the
joint
11. Type V
injury is a compression or
crush injury of the
epiphyseal plate with no
associated metaphyseal
fracture
.
This fracture is associated
with growth disturbances .
Initially, diagnosis may be
difficult, the diagnosis
depend mainly on clinical
features of premature closure
of physis ..& A typical
history of an axial load
injury.. These injuries have a
poor functional prognosis
..
12. clinical features As for any fracture.
X-ray It is difficult to assess as the physis is radiolucent and the
epiphysis is incompletely ossified.
1. The physeal widening of the gap
2. Tilting of the epiphysis
3. Repeating X ray within few days
4. Comparing the injured side with the normal
Treatment 1) Undisplaced → cast for 2-4 weeks
2) Displaced → reduce efficiently either by closed or open
reduction and internal fixation (it should be with smooth wires
or pins)
Complications
1. Deformities 2. Premature fusion (once the epiphyseal line is
closed that limb will remain short)
13. This male patient
,,13 years of age
who had a bullet
injury in the
antero –medial
side of the Lt.
Knee a partial
damage in the
upper epiphysis
causing genum
varum
14.
15.
16. Stress fractuers
This is an incomplete fracture in bones
A stress fracture occurs when a low
forces affecting repetitively for a
long period of time on a single bone ,
( usually seen in person who increase
his level of activity over a short
period of time)),, these injuries are
also known as "fatigue fractures."
Stress fractures are commonly seen in athletes
who run and jump on hard surfaces, such as
distance runners, basketball players, and
dancers. A stress fracture can occur in any
bone, but is commonly seen in the foot and shin
of the tibia
17. stress fractures can be considered an overuse injury
of a bone, The bones in the body are constantly
changing, responding to the work load that is placed
upon them, Bone is normally in homeostasis (homeo=
same + stasis=standing still), meaning that the natural
turnover of bone cells is in balance between osteoclast
activity (bone breakdown) and osteoblast activity (bone
creation). When bone is under stress, it undergoes
microscopic damage. Osteoclast cells are stimulated to
absorb bone, and the injured site is weakened. If a long
period of time elapses prior to the next injury,
osteoblast cells produce more bone cells to protect the
damaged area.
18. If there is not enough time for the osteoblasts to produce more
bone cells in the injured area; the micro fractures can join
together to form a large enough area to cause a stress fracture,
this fractures can also arise from normal use of a bone that's
been weakened by a condition such as osteoporosis.
Stress fractures are most common in the weight-bearing bones
of the lower leg and foot.
This is especially evident in the bones of the foot, leg, and
pelvis.
19. Cont. - Sterss Fr .
factor ‘s that can contribute to the development of a stress
fracture are dietary abnormalities and menstrual irregularities.
Because both factors contribute to bone health, any problems
with diet (e.g. poor nutrition, anorexia, bulimia) or
menstruation (amenorrhea) may place an individual at higher
risk for these injuries.
This is one reason that adolescent female athletes are at
particularly high risk for development of a stress fracture
.bones.
22. Pathologic Fracture
Definition
A pathologic fracture occurs when a bone breaks in an area that is
weakened by another disease process.
Causes
1) Tumour ;Either A) primary malignant bone tumours:
chondrosarcoma, osteosarcoma, Ewing's tumour
Or B) Secondary carcinomatus deposit :- breast, lung, thyroid,
kidney, prostate
2) generalised bone disease:- osteogenesis imperfecta,
postmenopausal osteoporosis, metabolic bone disease,
myelomatosis, polyocystic fibrous dysplasia, Paget's disease
3) local benign conditions: ;- chronic infection, solitary bone
cyst, fibrous cortical defect, chondromyxoid fibroma, aneurysmal
bone cyst, chondroma, monostotic fibrous dysplasia
23. Pathologic Fracture
Clinical features
Spontaneous or after trivial injury, with local and general features of fracture.
X ray shows fracture with diseased bone.
Management: Biopsy is needed.
Principals of fracture treatment are the same mostly by
internal fixation supplemented by cement.
Chemotherapy & radiotherapy may be added.
Prophylactic internal fixation
If a focus of metastasis with destructive features is shown in a long bone by
an x ray, an internal fixation should be done even if there is no fracture
because you expect that this may fracture
soon or later