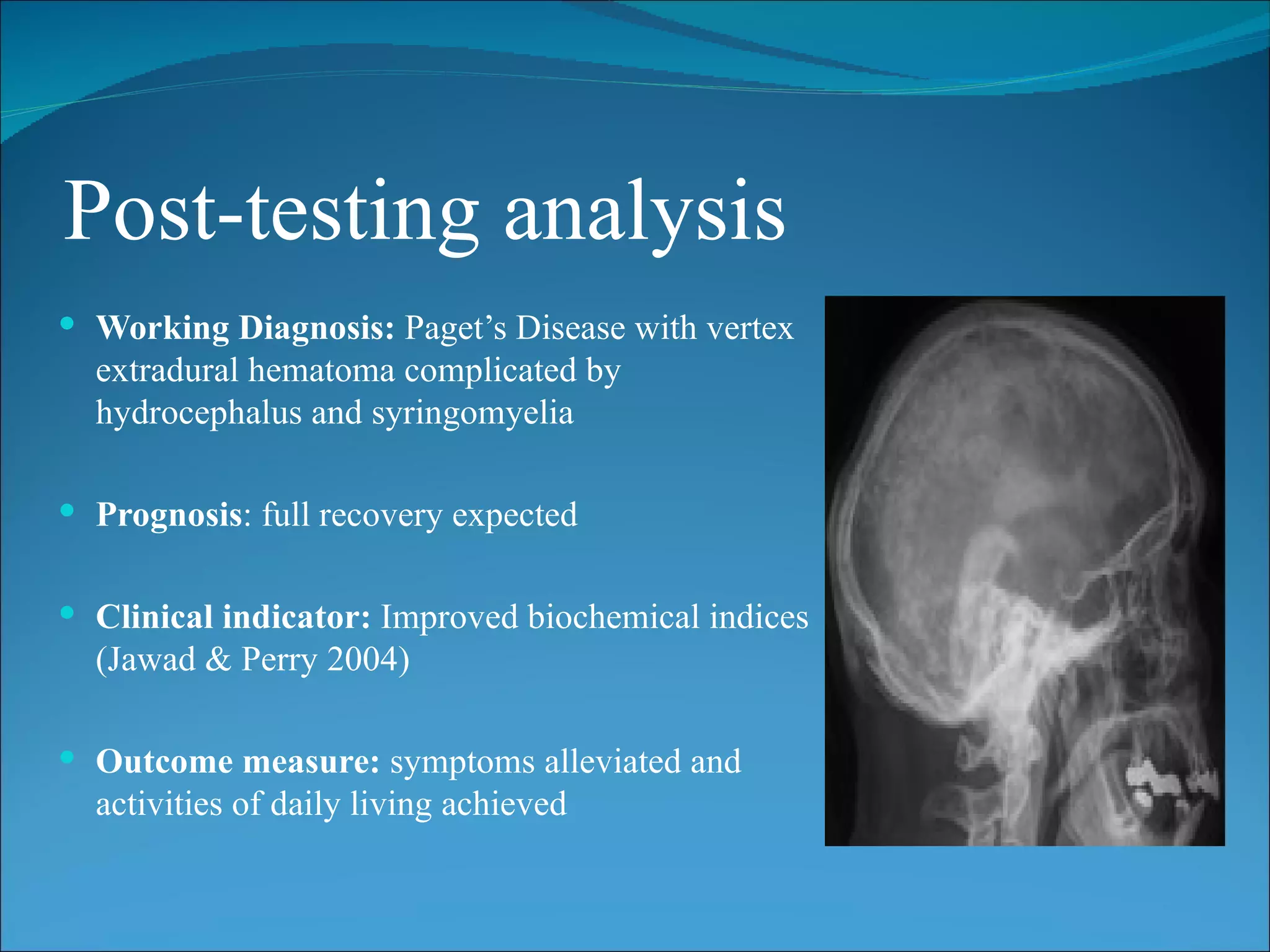
This case study describes a 48-year-old woman presenting with Paget's disease, a bone disorder causing abnormal bone growth and structure. She suffered a fall resulting in a skull fracture and extradural hematoma. Imaging showed signs of Paget's disease including widened skull bones. She underwent surgery to evacuate the hematoma. Treatment goals were to improve symptoms, prevent complications, and achieve remission through pharmacologic therapy and encouraging compliance. Outcomes included full recovery and meeting treatment expectations.