02 jonathan olesu - mouth guards and mouth protection
1. MOUTH GUARDS AND MOUTH
PROTECTION
By: Jonathan Olesu
UGDS, Class of 2012
2. Outline
Introduction
History
General Considerations
Function of Mouth Guards
Indications and Contraindications
Materials for Making Mouth Guards
Types of Mouth Guards
Design Specifications and Dimensions
How Mouth Guards Work
Use and Care Instructions
Setbacks
Other Mouth Protection Devices
Conclusion
References
4. Definitions
Mouth protection basically involves all the devices, substances and measures
put in place to prevent injury of any form to the oral cavity and its related
structures.
The injury may be:
Pathological
Traumatic
A mouth guard (MG) is a resilient intraoral device worn during participation in
contact sports to reduce the potential for injury to the teeth and associated
tissue (Mosby’s Dental Dictionary, 2004).
5. How Can the Mouth be
protected?
Protection implies prevention, rather than cure.
Personal oral hygiene and professional care like scaling and polishing can
sufficiently protect the mouth against pathological injury.
Protection against trauma is done only when mouth injury is anticipated
When traumatic oral injury is anticipated, a mouth guard is the most effective
means of protection.
6. Increasing number of participation in sports, and attendance to health clubs
and gymnasiums, implies a corresponding increase in the risk of trauma.
This calls for a concomitant increase in the adoption of protective means. The
use of the mouth guard in particular is on the rise, as a result of this.
7. History of Mouth Guards
Never throughout history has a man who
lived a life of ease left a name worth
remembering.
Theodore Roosevelt
8. The MG has had a long and dramatic timeline
Exact origin of the idea of mouth guard is not known
As “necessity is the mother of invention” would have it, boxers were the first to
employ the idea of mouth protection against trauma.
They were then called gum shields.
Innovative but crude; being manufactured from cotton, tape, sponge, or small
pieces of wood
These were prepared by the boxers themselves or their trainers.
9. Problems with the First Gum
Shields
They were not very effective
They were uncomfortable to wear
They had no means of retention
They were not reusable
They were not hygienic to use
Were not standardized
Impaired breathing and speech
Because of the above reasons, gum shields were not popular.
10. 1982– Woolf Krause
Seeing the problem, Woolf Krause, a British dentist based in London, began to
fashion mouthpieces for boxers in 1892
Krause’s mouth guards were manufactured from gutta-percha, a natural plant
resin
He made the rubber into single strips which he placed personally on the
maxillary incisors of boxers just before they entered the ring
Krause’s appliance was popular among amateur boxers.
Professional boxing mangers refused it because they thought it was an added
unfair advantage
11. Other Claims to Developing
Mouth Guards
Early 1900s: Jacob Marks created a custom fitted mouth guard in London.
1916: Thomas Carlos (USA) claimed he made his first customized mouth
guard which was used by a professional athlete.
1919: Allen Franke (USA) claimed he also made his first custom mouth guard
for a professional boxer.
12. The Breakthrough
All this while, mouth guards had not been made legalized
In 1927, there was a professional boxing match between Jack Sharkey and
Mike McTigue
Neither of them wore a mouth guard
McTigue broke his tooth and cut his lip. He was forced to forfeit the match due
to the bleeding
After that match, mouth guards were legalized for professional sports
13. The American Dental Association (ADA )continued to promote the use of
mouth guards from the 1940s onwards.
In the later 1960s and early 70s, the ADA and National Collegiate Athletic
Association (NCAA) in the United States made mouth guards mandatory in
college football.
Currently, the ADA recommends mouth guards be used in 29 sports:
acrobatics, basketball, bicycling, boxing, equestrian, football, gymnastics,
handball, ice hockey, inline skating, lacrosse, martial arts, racquetball, rugby,
shot putting, skateboarding, skiing, skydiving, soccer, softball, squash, surfing,
volleyball, water polo, weightlifting and wrestling.
15. Injury to the mouth may come in the form of trauma, inflammation, or other
pathological processes.
Trauma to the mouth can result in several forms of injury.
The exact form of injury that results from a traumatic episode depends on
several factors including; direction of force, intensity of impact and the tissues
involved.
16. Types of oral injury
Fractures:
Concussion
Subluxation
Extrusive luxation:
Lateral luxation:
Intrusive luxation
Avulsion
Contusion
Abrasion
Laceration
Concussion
Tempromandibular joint (TMJ) dislocation:
All the injuries mentioned above can be prevented or reduced in severity by a
mouth guard.
18. Prevent hard and soft tissue injury
Prevent concussions and TMJ dislocation
Provide psychological motivation
19. Indications of a mouth guard
Who should were a mouth guard?
When should it be worn?
20. For individuals who are at risk of trauma to the face or mouth
Sporting activities as mentioned earlier. Both professional and amateurish.
Children during casual play
Patients with increased overjet
22. When there is an active unresolved pathological oral condition.
If a patient is wearing a fixed orthodontic appliance some mouth guards are
contraindicated.
Patients with TMJ disorders.
Patients with severe malocclusion. This arrangement of teeth may not allow
the MG to function properly.
24. Earliest gum shield users made them from
cotton, tape, sponge, or small pieces of wood
Several materials have been used to manufacture mouth guards:
Ethylene vinyl acetate (EVA): Commonest
Latex rubber
Acrylic resin
Polyurethane
26. In simple terms EVA
Is highly flexible
Delivers high cohesive strength and compatibility
Ensures excellent adhesion to a wide range of substrates
Is highly resistant to rupture
Has good tear resistance
Is tough and can last long under constant stress
Is odourless
Resistant to ultra-violet radiation
Is biocompatible
All the above make EVA a good shock absorber
28. There are three main types of mouth guards. These types emerged based on
the processes involved in their fabrication and how customized they are for an
individual:
1.Stock Mouth Guards
2.Boil and Bite Mouth Guards
3.Custom Made Mouth Guards
29. Stock Mouth Guards
These are mouth guards that are pre-formed in the factory and are made
available as over-the-counter devices.
Once bought, they can be fitted immediately
Fabrication:
Factory-made
Different shapes, sizes and colours.
Advantages:
Easy to access and use.
Least cost of all mouth guards
They are versatile and allow for easy addition of technological advancements.
30. Disadvantages:
Inadequate fit
Bulky, making them uncomfortable.
Short life span.
Significant amount of effort required to retain in position especially for long
durations. Focusing on the game is difficult.
Speech and Breathing impairment
Recommendation:
Affordable, but ineffective option
Not recommended by dentists
31. Boil-And-Bite Mouth Guards
Currently the most widely used on the market
Fabrication:
They come in a form similar to plain stock mouth guards
Prepared by user: BoilBiteMould
Advantages:
Do not require much expert technique to prepare.
Provide better retention than stock mouth guards.
Versatile and allow for easy technological advancements.
More affordable than custom mouth guards.
32. Disadvantages:
The fit is not ideal.
Research has shown that most mouth-formed mouth guards are under-
extended.
They have the risk of becoming non uniform, because they are moulded
hurriedly with the hands and bite.
33. Recommendation:
85-90% of all mouth guards being used currently is of the boil-and-bite type
Mouth guards have a “not so good” name– because of boil-and-bite mouth
guards.
Most controversial
Claims that they can be better than custom mouth guards
Not prepared by dentists
Manufacturers claim good dentists are behind their good products.
34. Custom Mouth Guards
Dentists’ choice
Fabricated and delivered by the dentist
Currently provide the best fit.
The highest level of protection and comfort are provided by this type of mouth
guard.
A detailed fabrication process will be given
35. Fabrication of Custom Mouth
Guard
There are Five (5) main steps:
Diagnosis
Impression
Laboratory Fabrication
Trimming and polishing
Placement and Occlusal Equilibration
36. Diagnosis:
1.
History, Examination, Investigations
Some questions that need to be answered:
Does the client present with cavities and or missing teeth?
Does the client have any history of previous dental injury or concussion?
Is there a prospect of an eruption?
Will the design of the mouth guard be appropriate for the level of
competition being played?
Is the client undergoing orthodontic treatment?
Has the client ever used any mouth guards? How successful were they?
Can the patient afford and maintain the device?
37. Impression:
1.
Very important step. Will determine fit.
Impression is taken after all treatments have been done.
After the impression, major changes like restorations, prosthesis, medical
treatment, surgeries or extractions are not made
Must be made for both arches
The most common impression material used for mouth guards is silicone
impression material
All precautions required for taking a good impression apply.
38. Laboratory Fabrication:
1.
Impression is poured immediately with hard die stone.
Outline the “Mouth guard bearing area”.
The model is trimmed to remove excess stone.
The base is preferably left thin up to about five millimeters
Model is then left to dry
Model is coated with a lubricant or separating medium
The lubricant of choice is the orthodontic model soap (Padilla, 2005).
The model is soaked in the soap for one hour and dried with a towel.
It is now ready for construction of the mouth guard.
39. Two types of machines and thus two methods can be used to adapt the
thermoplastic material unto the stone model
Method 1: Vacuum-formed mouth guards
A through-and-through hole is made in the center of the model not covered by
the pencil mark.
A sheet of EVA is heated in a vacuum-forming machine and then adapted to
the stone model with negative pressure.
When the material has softened enough and is mouldable, it is lowered quickly
onto the model on the platform.
The machine sucks air from between the EVA material and the model. This
adapts the material to the model
40. The setup is then removed and the model and thermoplastic material allowed
to cool to room temperature.
After cooling, the mouth guard is removed for trimming and polishing.
The main limitation of this of method is that it does not adequately support
adding several sheets in layers.
41. Method 2: Pressure-laminated mouth guards
This is the better and more commonly used method.
Uses specialized machines that apply high heat and pressure
Allows for lamination of multiple layers
To achieve 3-4mm of mouth guard thickness, two sheets of EVA each of 3mm
are used
First, a 3-mm sheet of EVA is placed in the disk positioning ring of the machine
and clamped in position
The model is placed on the platform below this ring, slightly offset lingually.
42. The heater is brought over the model to heat the sheet of EVA until soft
enough to slump downwards and touch the model.
The pressure is then activated with a button which brings down a pressure
chamber on the model, adapting the EVA to it. The button is held in position
until a signal on the machine shows that it can be released.
Once released, the EVA material is allowed to cool to room temperature.
The EVA is removed and trimmed grossly with a trimming knife.
The process is repeated with a second layer of EVA. Care should be taken to
adequately heat this layer so that it can bind with the first layer.
The EVA is allowed to cool and then trimmed and polished.
43. Trimming and Polishing:
1.
Gross trimming: Trimming knife to remove excess material.
The buccal extension is trimmed up to the height of
An acrylic polishing bur is then used to smoothen the edges of the appliance
Wax removal fluid can be used to give it luster.
44. Placement and Occlusal Equilibration
1.
With the mouth guard in place, the patient should feel comfortable when biting.
The occlusion must be balanced.
To achieve this, the posterior portion of the appliance is slightly warmed. It is
placed in the mouth and the patient is made to bite down gently into habitual
occlusion.
All impinging areas can be trimmed at the chair side.
At this point, major adjustments should be avoided.
The patient is given instructions on how to care for the appliance, and then
discharged.
45. Advantages of Custom Mouth Guards:
They provide the best fit, since they are customized.
The client gets the benefit of having total oral care.
They do not interfere significantly with speech or breathing.
Personalization like incorporating a name can be made.
Disadvantages of Custom Mouth Guards:
Most expensive type.
Least versatile and do not allow many advanced technological advancements.
46. Cast Model Model trimming Sheet of EVA locked into place
EVA slumping to touch model First layer completed Finished appliance
49. Scott et al., 1994
It should enclose the maxillary teeth to the distal surface of the second molar,
or cover all the teeth.
Thickness should be 3 mm on the labial aspects, 2 mm on the occlusal aspect,
and 1 mm on the palatal aspect.
The labial flange should extend to within 2 mm of the vestibular reflection.
The palatal flange should extend about 10 mm apical to the gingival margin.
The edge of the labial flange should be rounded in cross section whereas the
palatal edge is tapered.
Even when a single maxillary protector is constructed it should be articulated
against the matching mandibular model to give optimum comfort.
50. Greasly et al., 1998
Found that the following guidelines should be added:
Multiple layers of EVA should be utilized to build a 5 mm thick layer in the
thicker parts of a custom made protector.
The protector should be extended to at least behind the first molar or as far
along the second molar to provide wearer comfort.
51. The Perfect Mouth Guard:
It should be made from the best elastic and strong material available (currently
EVA)
It should be constructed to the appropriate dimensions and shape as stated
above.
It should provide an accurate fit.
Adjustments must easily be made without reducing effectiveness of the
appliance.
It should not interfere with speech and breathing.
It should be easy to fabricate.
It should be effective. That is, it should actually work.
It should not be bulky.
It should not interfere with the occlusion of the individual wearing it.
It should be durable and last long.
It should not cause damage to the oral tissues
It should be easy to clean.
It should be biocompatible.
52. HOW MOUTH GUARDS
WORK
Certainly, these little appliances cannot
protect against a blow from a heavy-weight
champion… or can they?
53. How do mouth guards work?
They definitely do not feel like a cushion, and they do not feel like a metal
shied.
Dr Anthony Lovat, a dentist, mouth protection specialist, and founder of the
world’s biggest supplier of mouth guards, OPRA Mouthguards did a lot of
extensive work to publish exactly how mouth guards work.
Most of the information in this text is credited to him.
54. It’s not Magic; it’s Science
Three aspects of science have to be considered here, and these are
1.Time
2.Area
3.Elasticity
1.Time:
Damage is inversely proportional to duration of impact. This can be shown by
the equation:
Where f=force, m=mass, a=acceleration, v=final velocity, u=initial velocity and
t=time
55. Damage is reduced by lengthening the
time over which a force is applied.
The flexible and compressive EVA allows
the impacting object force to slow down
and reach a halt over a longer period of
time and hence the resulting transmitted
force is reduced.
1.Area:
Damage is inversely proportional to area
over which force is applied.
56.
57. Elasticity:
1.
One fundamental rule of physics is that energy cannot be created or
destroyed.
The mouth guard uses this principle in its function, by way of its elasticity.
Energy is absorbed by elastic change.
EVA will compress on impact and return to its original shape (if the distorting
force is within the mouth guard's elastic limit).
That compression and return takes energy. Because the material is made up
of atoms that have some free movement, the energy is used as kinetic energy
in compression and returning to original position.
The thicker the material, the more it can compress and the more energy it can
'absorb' from the impacting object.
58. The Fit
The better the fit, the better the appliance because retention is better.
A poor fit does not provide enough contact area and thus not enough shock
absorption.
A good fit also allows for easy breathing and speech.
59. How Mouth Guards Prevent
Concussions
Controversial
“ Concussion is a complex pathophysiological process affecting the brain,
induced by traumatic biomechanical forces”. International Symposium on
Concussion in Sport (2001)
Concussion typically involves temporary impairment of neurological function
that heals by itself within time, and that neuroimaging normally shows no gross
structural changes to the brain as the result of the condition
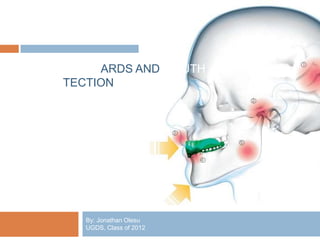
60. The mechanism of concussion is acceleration of the brain.
The brain is surrounded by cerebrospinal fluid, one of the functions of which is
to protect it from light trauma, but more severe impacts or the forces
associated with rapid acceleration may not be absorbed.
A force applied to the jaw can be transmitted to the brain by one of two primary
routes:
61. The diagram on the left is the path of the force when there is no mouth guard. The
one on the right illustrates what happens with a mouth guard in place.
64. Technological advancements are applied mostly to the boil-and-bite mouth
guards.
There is some skepticism concerning whether these features actually work, or
are just unnecessary luxuries.
65. Feature of a Modern Mouth
Guard
Multiple layers:
Gel-fit liner: It improves fit.
Shock transfer core: Uses an inner mould of
hard and semi thermoplastic material. It
transfers heavy anterior forces directly to
the strong multi-rooted molar teeth.
Air Spring Core™: This feature adds an
additional shock absorbing system within
the hard core of the molar area of the mouth
guard.
66. Magnetic Tethered Guard:
Flavours
Double Mouth Guard
Lip Protector
INSTA-FIT ™: Invented by Shock Doctor Company for
patients with braces who still require a mouth guard. It is
claimed that it adapts to changes in tooth position and
protects from lacerations.
Personalization: Some athletes prefer to customize their
appliances. Images or text can be incorporated into the
appliance.
67. POWRGARD® Modern Mouth Guard
Mouthguard
Personalization of MG
Double MG
70. Braces and Mouth guards:
Stock or Custom Mouth guards can be made for individuals with fixed
orthodontic braces.
The principles are that the mouth guard should not adapt to the teeth
or the brace itself, but be made with some space inside to allow
movement of the teeth.
This compromise in fit does mean the mouth guard may be somewhat
loose.
As teeth move, retention decreases
It would not be as loose as a self-boil mouth guard as it will be in
contact with the gums, and engage the natural undercuts of the mouth.
The improved adaptation to the palate will still mean that an athlete
can speak and breathe better than with a boil and bite mouth guard
and he or she will have protection against the brace or brackets
injuring the lips.
71. Children
Dental trauma may be due to sports,
falling at home, collisions
Peak period for trauma to the
primary teeth is 18 to 40 months of
age
Averagely 30% of such children
experience dental trauma
Two times more common in boys
72. Upper centrals are most commonly injured
Protruding incisors 2-3 times more commonly traumatized.
All children involved in contact sports should wear a mouth guard
Custom mouth guards are best
Mouth guards have to be changed to adapt to changing dentition
73. MOUTH GUARDS: USE AND
CARE INSTRUCTIONS
The Dos and Don'ts
Instructions are given by dentists or
manufactures
74. Mouth guards should be worn in practices first, as well as games.
The appliance should not be chewed on.
Rinse the mouth guard with cold water or with a mouth rinse before and after
each use.
It should be cleaned with toothpaste and a toothbrush or cleaned in cool,
soapy water followed by thorough rinsing.
The mouth guard should be stored and transported in a firm, perforated
container
Mouth guards should not be shared.
75. The condition of the mouth guard should be checked occasionally and
replaced if it has holes or tears, becomes loose, or irritates the teeth or gums.
If the mouth guard absorbs a strong blow, it may need to be replaced.
The material deteriorates and loses resilience over time. Therefore, they
should be replaced every two to three years. Earlier replacement is
recommended if any damage is detected.
They should be taken to every dental visit.
77. Speech:
Athletes may need to communicate.
A Custom Mouth guard provides a good fit an makes speech easier.
Breathing:
Optimum athletic performance requires unrestricted flow of air into the
lungs.
A well fitted custom mouth guard allows easy breathing.
Boil-and-bite mouth guards may inhibit breathing.
Double mouth guards impair breathing.
Comfort:
In truth, the ideal mouth guard is one that the athlete forgets he or she is
wearing.
Most publications show that the custom mouth guards are the most
comfortable to wear; but the recent technological additions make the boil-
and-bite mouth guards also equally comfortable.
79. Face Mask:
The face mask is basically a helmet with a spacy
metallic extension over the face. This puts the
entire head in a protective cage. It is used
mainly by football players. The main aim of the
face mask is to prevent maxillofacial injuries.
Though it provides a good barrier against injury
to the mouth, a mouth guard is still required to
ensure total mouth protection.
Lip Guard:
This device is also made from thermoplastic
material. It is more flexible than the mouth guard.
80. In Conclusion…
Every tooth in a man's head is more
valuable than a diamond.
Miguel de Cervantes, Don Quixote, 1605
81. Mouth protection is an important aspect of the health of every individual.
The importance of wearing mouth guards is now clear among professional
sportsmen.
The only debate now is probably whether the better choice is the traditional
dentist’s custom mouth guards, or the flashy, technologically improved but
more affordable boil-and-bite mouth guards.
Either way, the mouth guard has prevented oral injuries greatly over many
centuries and is definitely a field of dentistry worth exploring and perfecting
84. Andreasen J, Andreasen F, Andreasen L. Textbook and Color Atlas of
Traumatic Injuries to the Teeth. Blackwell Mungkar, Copenhagen. 2007. Pages
404-444.
Canadian Dental Hygienists’ Association. Information for Dental Hygiene
Clients: Mouthguard use and care. 2010.
Craig, G.R., Powers J.M. Restorative Dental Materials, 11th edition. Mosby
Inc, USA 2002. Pages 217-222
Craig RG, Godwin WC: Physical properties of materials for custom-made
mouth protectors, Mich Dent Assoc J 49:34, 1967
DeYoung AK, Robinson E, Godwin WC. Comparing comfort and wearability:
Custom-made vs. self-adapted mouth guards, American Dent Association
125:1112, 1994.
Langfitt TW. Measuring the outcome from head injuries. J Neurosurgery
1978;48:673–8
Lovat Anthony, BDS. How Mouth Guards Work. 2005. Pages 3-12.
Miloro Michael, Peterson’s Principles of Oral and Maxillofacial Surgery.
Second edition. B.C. Decker Inc, London. 2004. P327
Mosby’s Dental Dictionary, Mosby Inc. 2004.
85. Padilla R. A Technique for Fabricating Modern Athletic Mouthguards. Canadian
Dental Association Journal. Vol 44. No 5. May 2005.
Using Mouth guards to reduce the Incidence and Severity of Sports-related
Oral Injuries." Journal of the American Dental Association 137.12 (2006):
1712-1720
http://en.wikipedia.org/wiki/Mouth_guard
http://www.catalogs.com/info/bestof/top-10-mouth-guard-instructions
http://sportsmedicine.about.com/od/shop/tp/mouthguardpicks.htm
http://www.mogosport.com/mogo-technology
http://www.powrgardsports.com/index.php?technology
http://www.sportsdentistry.info/mouthguards.html
http://www.sportsdentistry.info/prevention.html