Downloaded 37 times


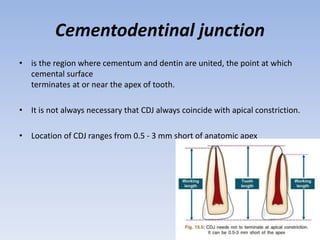






This document discusses methods for determining the working length in root canals, including definitions of relevant anatomical structures. It describes the cementodentinal junction and compares anatomical and radiographic apices. Electronic apex locators are discussed as an adjunct to radiography for accurately locating the apical constriction or cementodentinal junction. Advantages include objective measurements with high accuracy, especially useful when radiographs are limited. Proper use and limitations of electronic apex locators are also outlined.











































































































