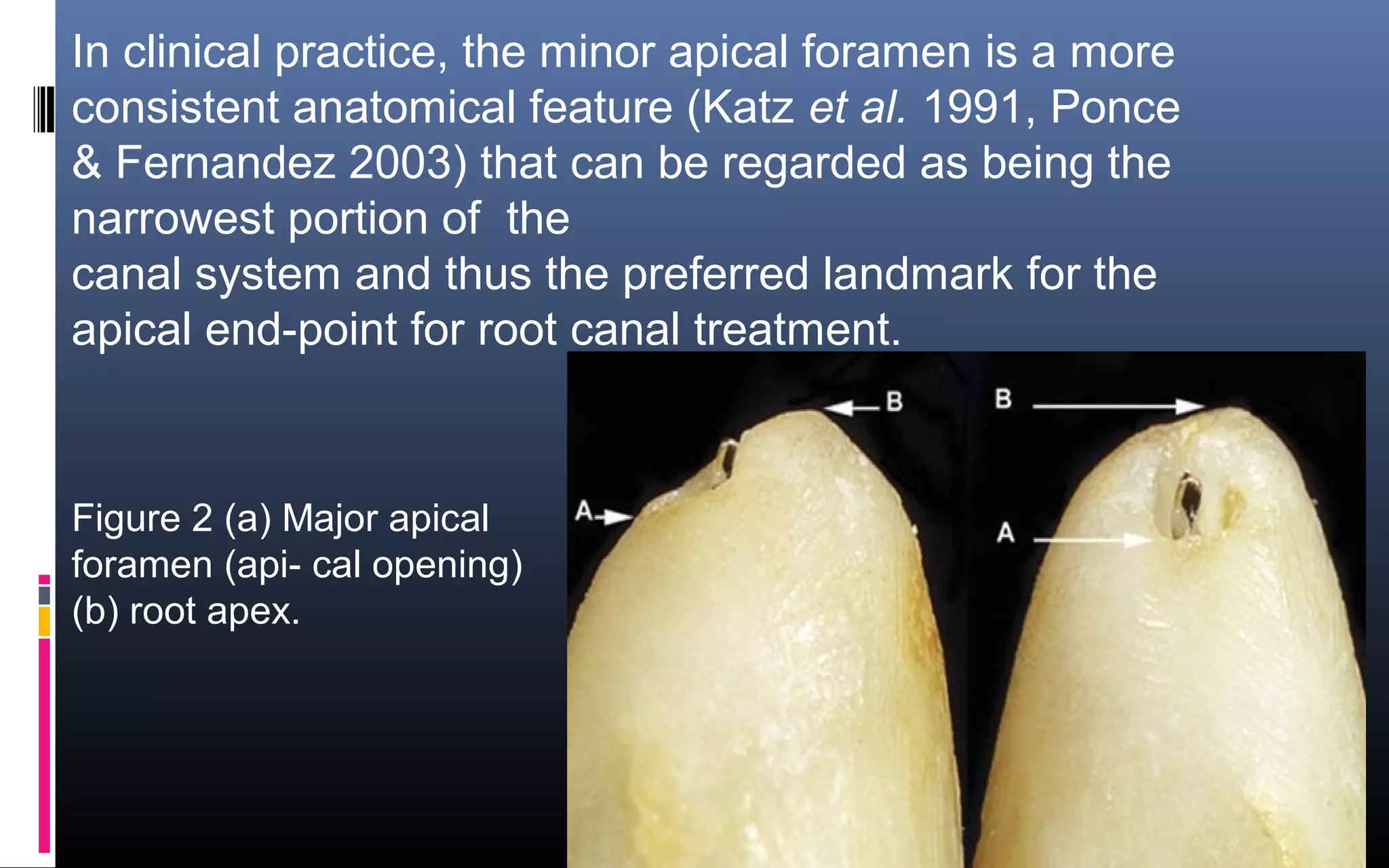
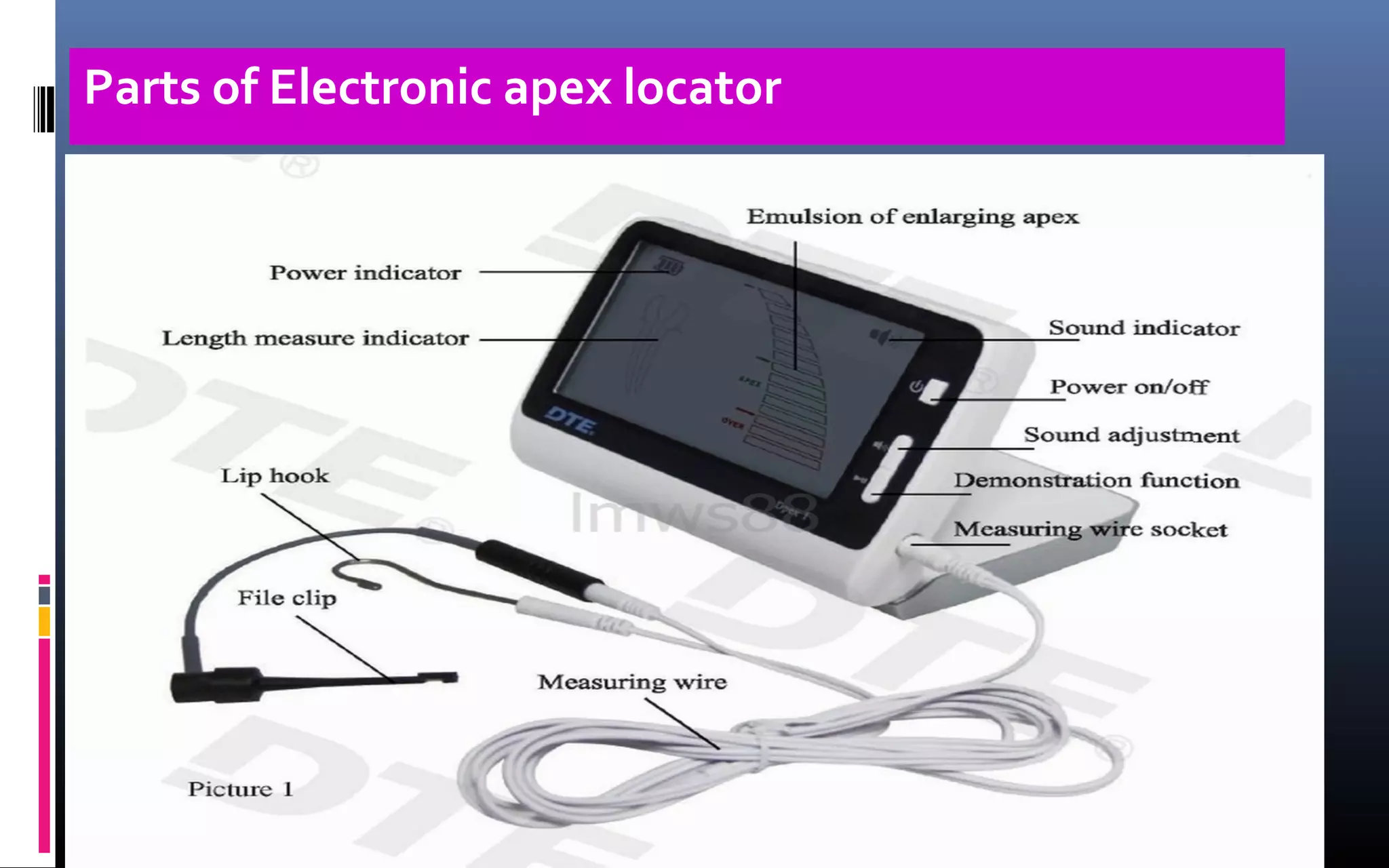
The document provides an extensive overview of electronic apex locators (EALs), including their definitions, historical developments, and capabilities in determining root canal lengths with high accuracy. It discusses the limitations of traditional radiographic methods, outlines the anatomy of the apical foramen, and describes how to properly use EALs while avoiding false readings. The importance of integrating radiographs with EAL findings to improve endodontic outcomes is emphasized.
















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
