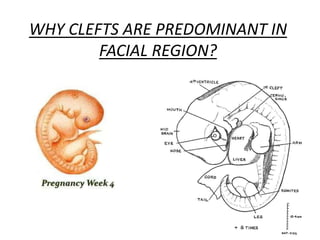
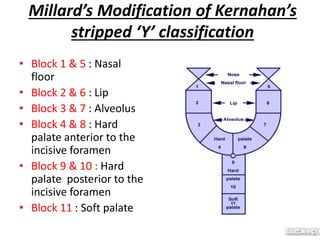
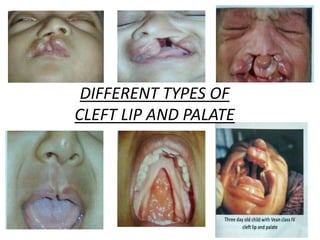
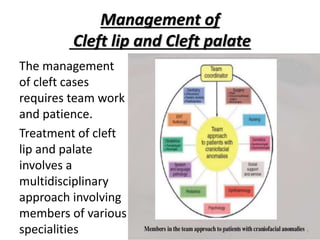



The document provides information on cleft lip and cleft palate including definitions, incidence rates, development, classifications, problems associated, and treatment protocols. It defines cleft lip as an opening in the upper lip and cleft palate as an opening in the roof of the mouth. Treatment is a multidisciplinary approach involving surgery to repair the cleft, orthodontics to align teeth and jaws, and speech therapy. Management occurs over many years from infancy through adulthood to address dental, esthetic, speech and other issues.