Downloaded 250 times

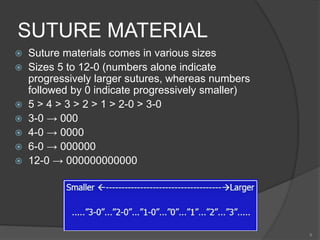


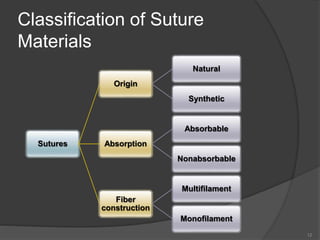
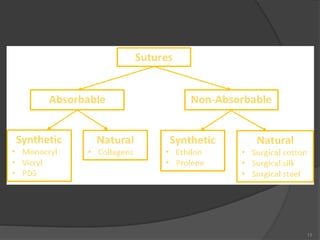
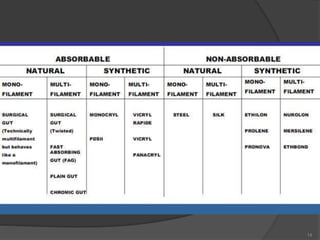










The document discusses suturing techniques and principles. It begins by stating that proper surgical closure using sutures helps reduce postoperative infections by approximating tissues and preventing fluid accumulation. Sutures have been used since prehistoric times, originally made from plant or animal materials attached to bone or metal needles. The document then covers suture materials, both absorbable and non-absorbable varieties, as well as monofilament and multifilament types. It provides details on specific commonly used suture materials like silk, catgut, nylon and polyglycolic acid. Principles of proper suturing technique are also outlined.












































































