Downloaded 3,545 times
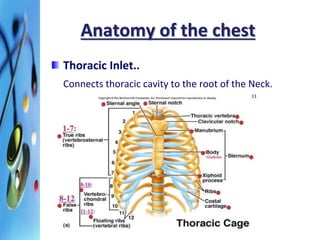
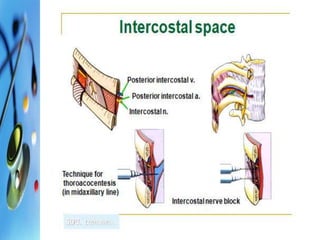
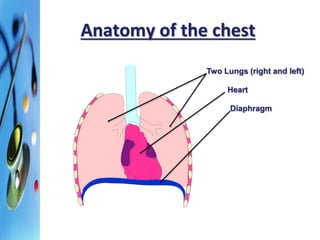
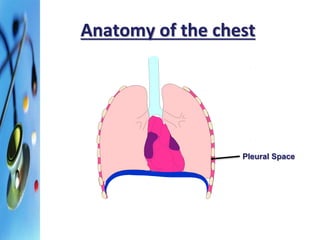
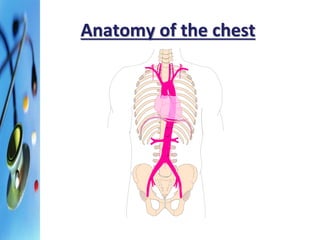
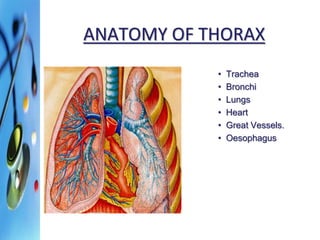

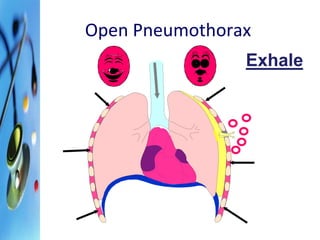
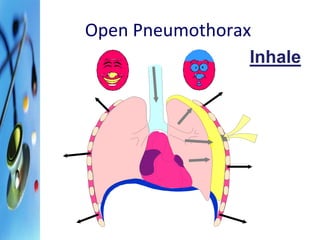
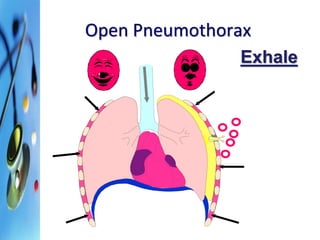
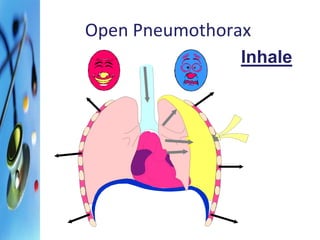
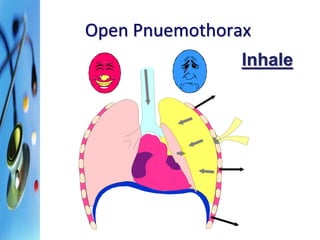
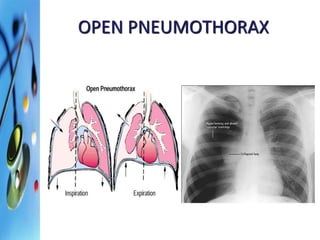
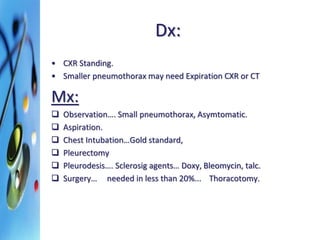

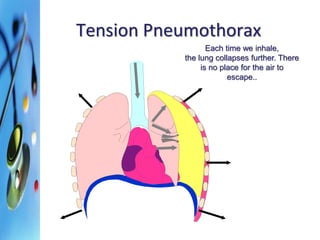
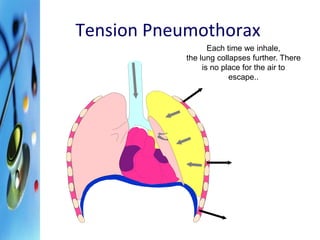
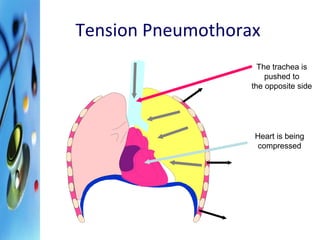
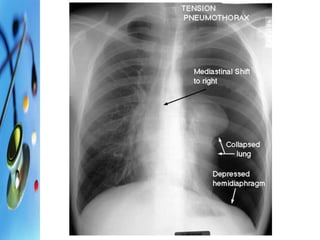
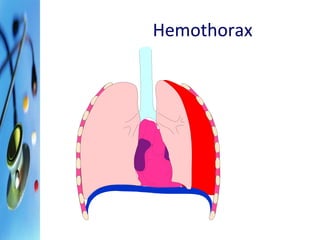
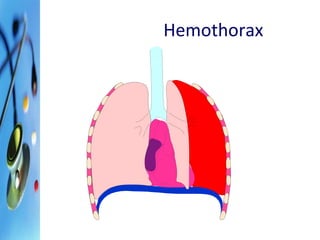
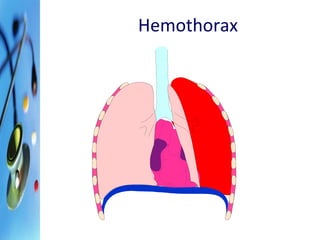
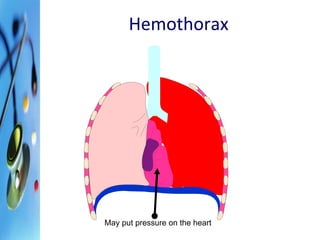
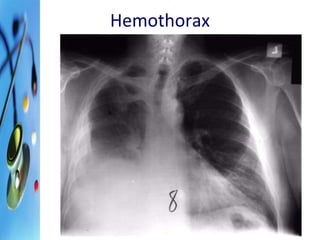
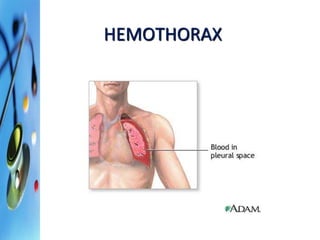
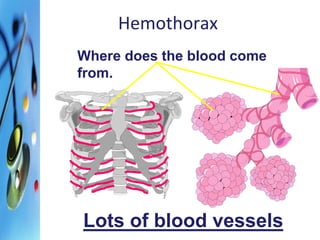
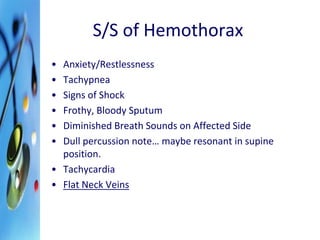
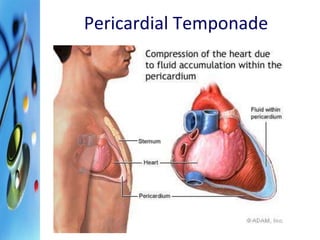
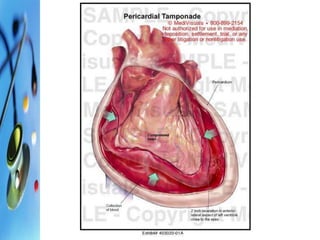


This document provides an overview of chest trauma, including the anatomy of the chest, causes of chest injuries, types of chest injuries, and treatments. It begins with the objectives and anatomy of the thorax. The main causes of chest trauma are then discussed as blunt trauma, penetrating trauma, and compression injuries. Various chest injuries are described in detail such as rib fractures, flail chest, pneumothorax, hemothorax, pulmonary contusion, and pericardial tamponade. The treatments for each type of injury are also outlined. The document provides a comprehensive review of chest trauma for medical professionals.

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















