Downloaded 576 times
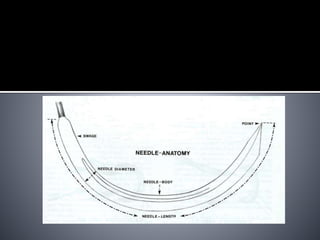
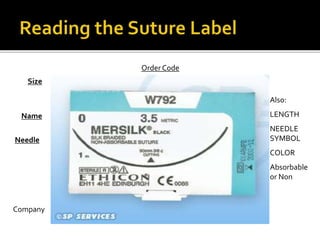
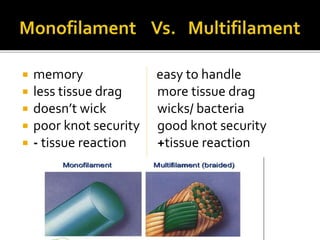
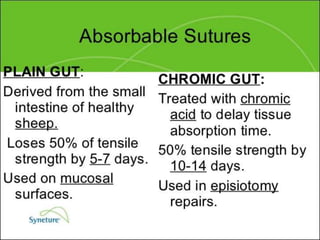
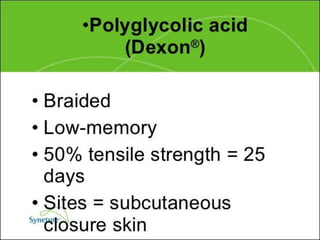


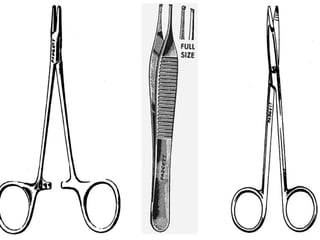

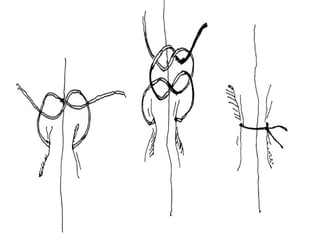
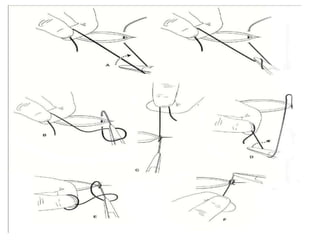
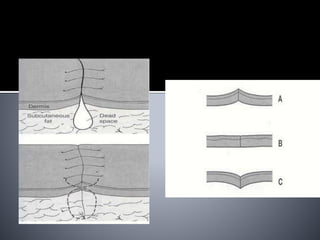
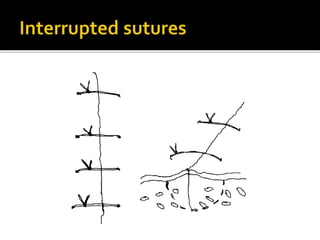
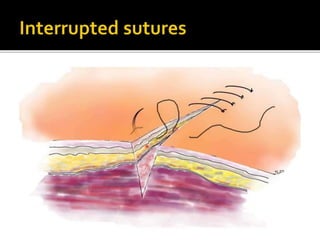
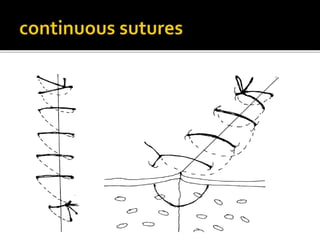
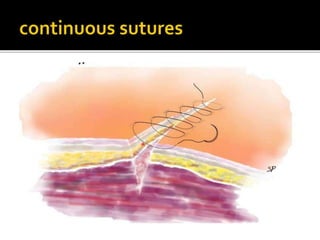
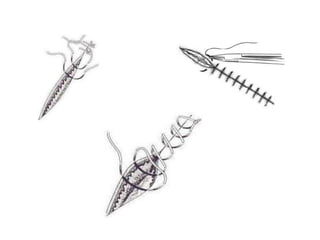
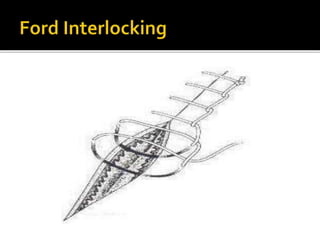
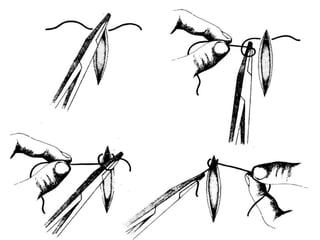


The document discusses surgical sutures and needles. It covers their properties, types, uses and techniques for placement and removal. Some key points include: 1) Sutures must be pliable, sterilized, non-reactive and have adequate tensile strength for wound healing. Absorbable sutures like Vicryl degrade over time while non-absorbables like nylon are permanent. 2) Needles come in different shapes, sizes and points for various tissue types. They have an eye, body and point. 3) Common suture techniques include simple interrupted, continuous, mattress and subcuticular closure. Knot security requires at least 4 throws. 4)























































































