Downloaded 1,329 times

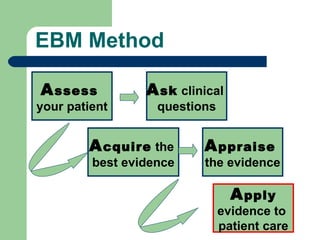
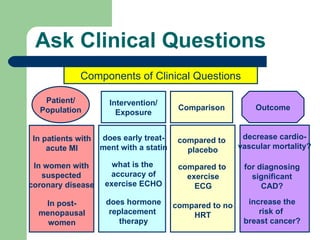

This document provides an overview of an evidence-based medicine (EBM) curriculum consisting of 3 modules: 1) Introduction to EBM, 2) Applying EBM to diagnosis, and 3) Applying EBM to treatment. It was prepared by faculty at Emory University School of Medicine and discusses the history and importance of EBM, how to formulate clinical questions and find the best evidence to answer them, and how to critically appraise and apply evidence to patient care.