Downloaded 128 times

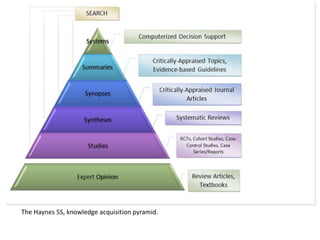









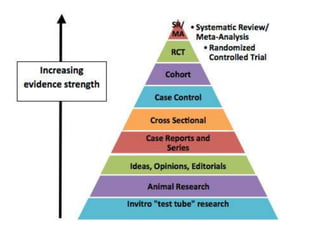
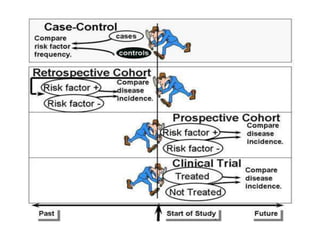
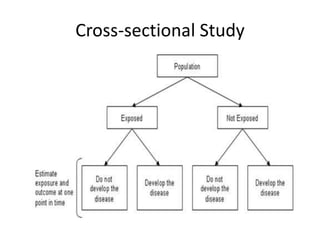



This document discusses the principles of evidence-based medicine (EBM), highlighting its definition, hierarchy of evidence, and the significance of integrating clinical research with physician experience and patient preferences. It covers various types of clinical questions, evidence sources, and the process of utilizing medical literature for optimal patient care, including practical examples and guidelines for searching. The importance of systematic reviews, particularly through organizations like the Cochrane Collaboration, is emphasized for making informed health interventions.