SS/EBM/IKA-UDIP-2010
Dr. Benjamin Spock:
Babyand Child Care
Later evidence indicates that prone position is a
an significant risk factor for SIDS
(sudden infant death syndrome)
“I think it is preferable to accustom a baby to sleeping
on his stomach from the start of he is willing. He may
change later when he learns to turn over”.
SS/EBM/IKA-UDIP-2010
Diagnosis
Patient with complaint
History
Physical
Simpletest
• Specific test: If the test (+) what is the probability that the
patient has the disease?
Yes or no answer
Predictive value is the most important
The spectrum of the presentations must resemble that in practice
Studies to be searched: Diagnostic tests
7.
SS/EBM/IKA-UDIP-2010
Treatment
Patient with certaindiagnosis: best treatment?
Is drug X more effective than Y?
Focus on the clinical outcome, rather than its explanation
(biomolecular markers, etc)
Yes or no outcome most useful
Not in studies with “idealized” subjects
Px with DM are frequently have hypercholesterolemia,
obese, hypertension, etc
Sudies to be searched: RCT
8.
SS/EBM/IKA-UDIP-2010
Prognosis
Usually in cohortstudies
To inform about the fate of the patient
Absolute risk is more important than relative risk
Absolute: Your risk of having second stroke in 1
year is 30%
Relative: Your risk of having second stroke in 1
year is 2 times than in non-smokers (RR = 2)
Studies: Cohorts, case controls
9.
SS/EBM/IKA-UDIP-2010
Pros : “Newparadigm in medicine”
“Extraordinary innovations,
only 2nd to Human Genome Project”
Cons : New version of an old song
„Fair‟ : Nothing wrong with EBM, but:
• Be careful in searching evidence
• Meta-analyses, clinical trials, and all study results
should be critically appraised
Keyword for EBM:
Methodological skill to judge the validity
of study reports (Re. Andersen B: Methodo-logical errors
in medical research, 1989)
10.
SS/EBM/IKA-UDIP-2010
EBM & ClinicalEpidemiology
Fletcher & Fletcher: CE = The application of epidemiologic
principles in problems encountered in clinical medicine
Sackett et al: CE = The basic science for clinical medicine
Much resistance by experts
EBM: In principle – no one disagree
All major medical journals have adopted EBM
Centers for EBM all over the world
11.
SS/EBM/IKA-UDIP-2010
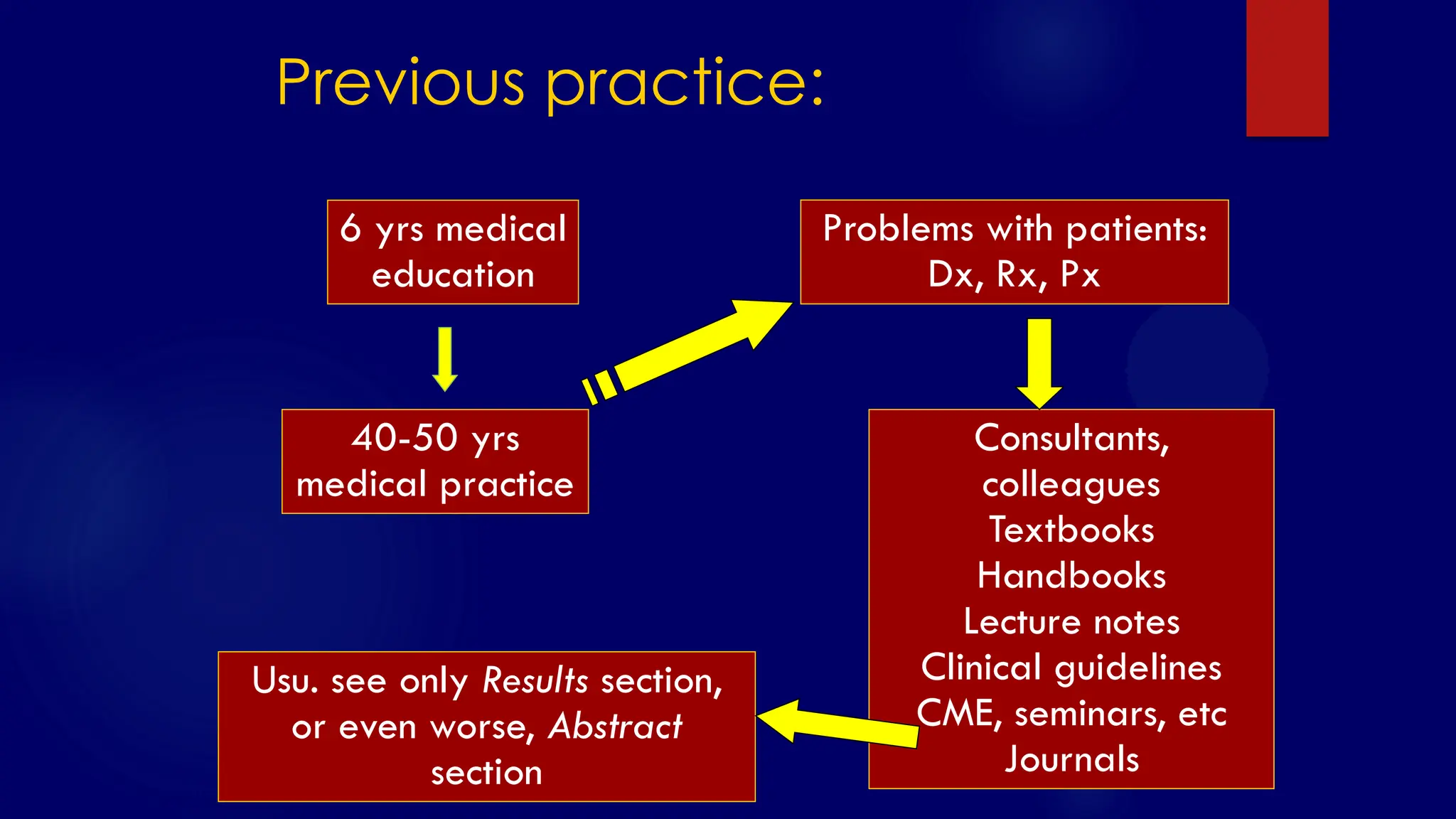
Previous practice:
6 yrsmedical
education
40-50 yrs
medical practice
Problems with patients:
Dx, Rx, Px
Consultants,
colleagues
Textbooks
Handbooks
Lecture notes
Clinical guidelines
CME, seminars, etc
Journals
Usu. see only Results section,
or even worse, Abstract
section
SS/EBM/IKA-UDIP-2010
The results….
Opinion-based medicine
Steroidinj. in prematures to prevent RDS
Routine episiotomy
Routine circumcision
Antibiotics for flu-like syndrome
Use of immunomodulators
“Skin test” before antibiotic injection
Routine chest X-ray for pre-op preparation
CT scan after minor head trauma
14.
SS/EBM/IKA-UDIP-2010
What is
Evidence-based Medicine?
“Theconscientious, explicit, and judicious use of current best
evidence in making decisions about the care of individual
patients”
“Pemanfaatan bukti mutakhir yang sahih dalam tata laksana pasien”
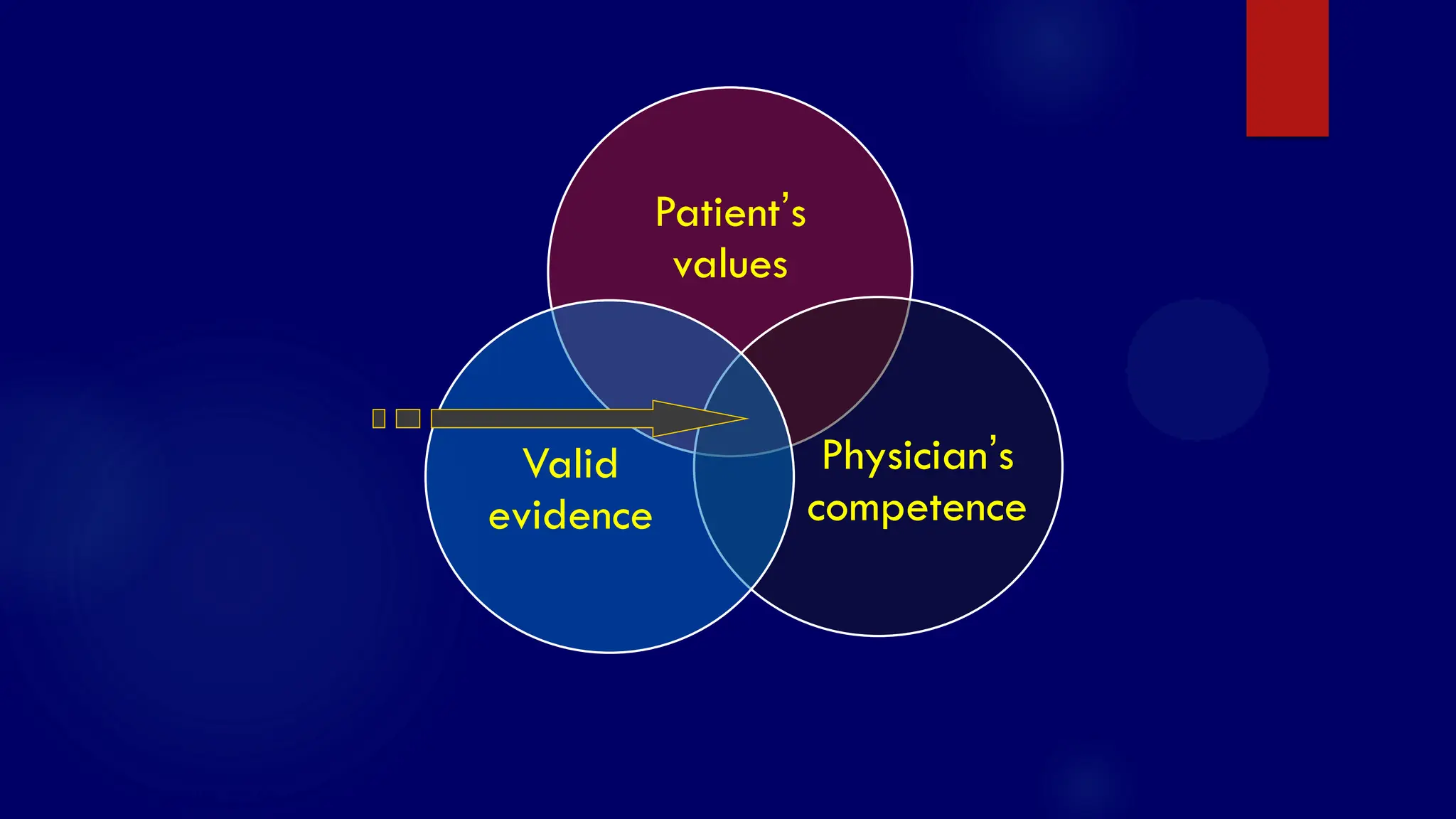
Integration of
• physician‟s competence
• valid evidence from studies
• patient‟s preference
15.
SS/EBM/IKA-UDIP-2010
Why EBM?
Information overload
Keepingcurrent with literature
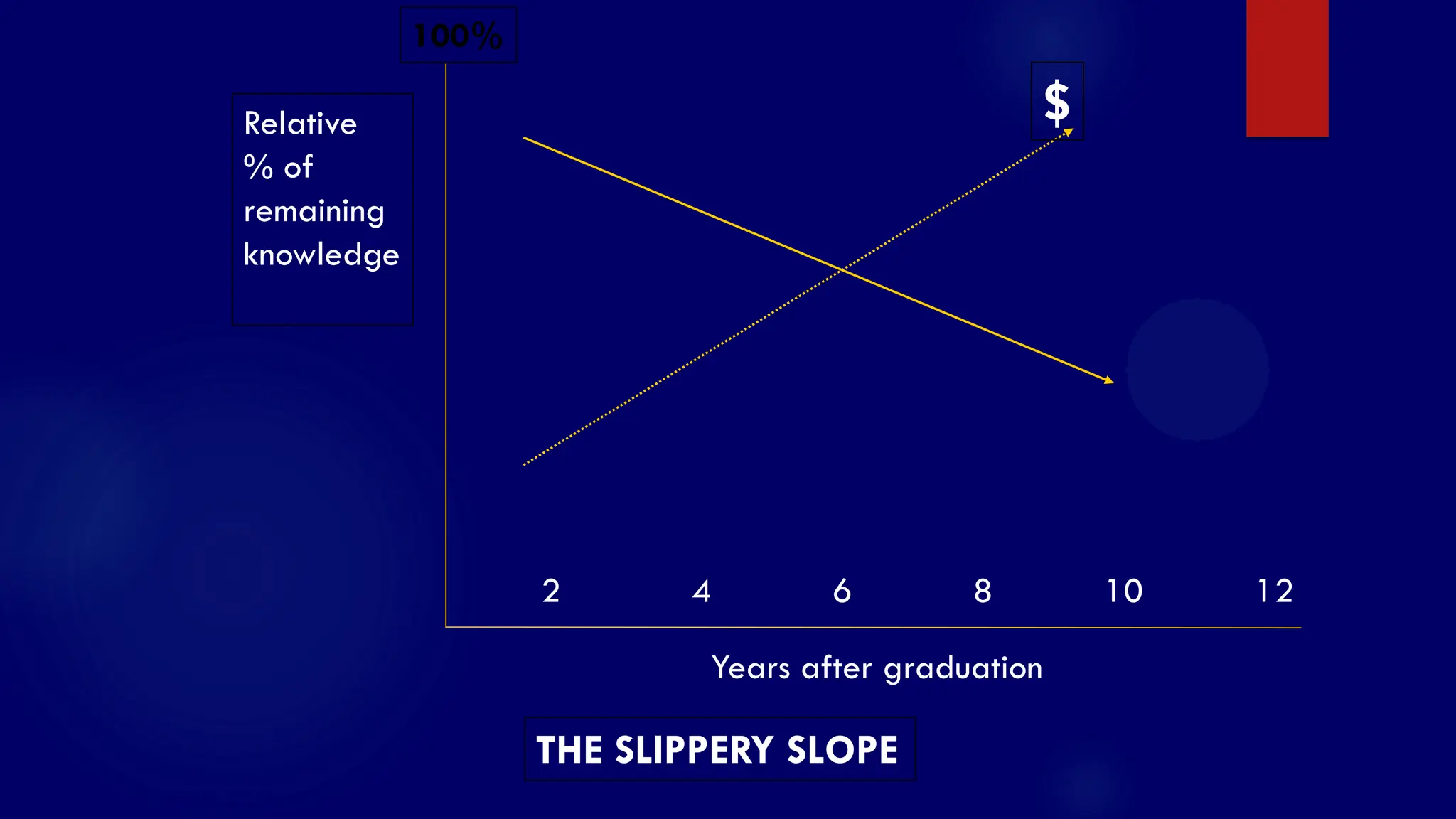
Our clinical performance deteriorates with time (“the
slippery slope”)
Traditional CME does not improve clinical performance
EBM encourages self directed learning process which
should overcome the above shortages
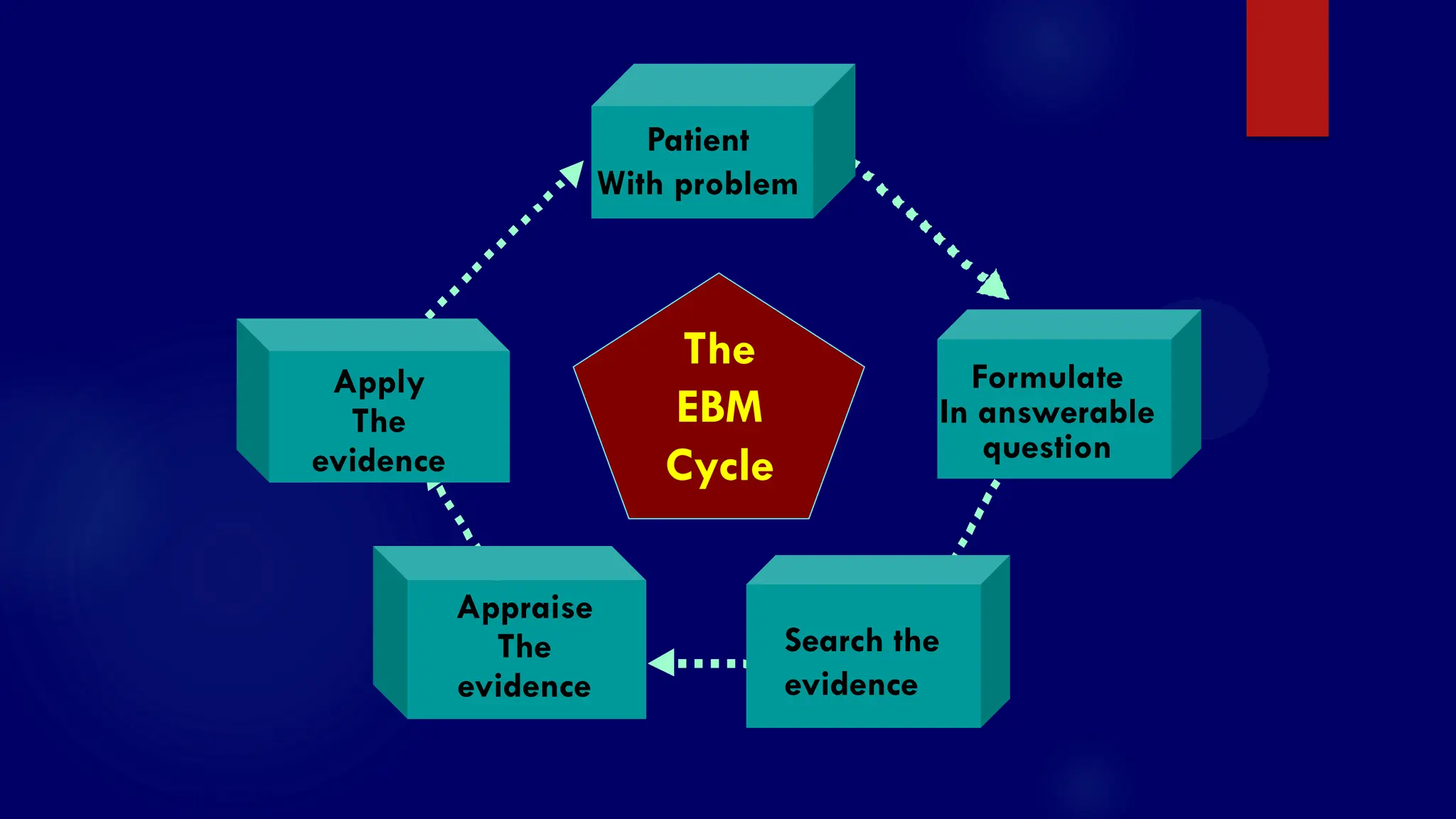
SS/EBM/IKA-UDIP-2010
1. Formulate clinicalproblems in answerable questions
2. Search the best evidence: use internet or other on-
line database for current evidence
3. Critically appraise the evidence for
Validity (was the study valid?)
Importance (were the results clinically important?)
Applicability (could we apply to our patient?)
4. Apply the evidence to patient
5. Evaluate our performance
Steps in EBM practice
VIA
SS/EBM/IKA-UDIP-2010
A 2-yearold boy presented with 6-day high
fever, conjunctival injection without secretion, skin
rash> blood test shows leukocytosis, high ESR,
CRP +++. He was suspected to have Kawasaki
disease. The pediatrician is aware of the use of
immunoglobulin to prevent coronary involvement,
but uncertain about the dosage or recent
developments.
SS/EBM/IKA-UDIP-2010
Other examples
In youngwomen with solitary thyroid nodule, can USG,
compared with biopsy, differentiate between benign
from malignant? (Diagnosis)
In women systemic lupus erythematosus, is history of
congestive heart failure, compared with no heart
failure, worsen the prognosis? (Prognosis)
In women with history of eclampsia, would
administration of low-dose aspirin during pregnancy
prevent eclampsia? (Prevention)
26.
SS/EBM/IKA-UDIP-2010
Four elements of
goodclinical question: PICO
The Patient or Problem
The Intervention / Index / Indicator
Comparative intervention (if relevant)
The Outcome
27.
SS/EBM/IKA-UDIP-2010
Four elements ofa well constructed
clinical question: PICO
P I C O
The main
intervention
considered
The
alternative
to compare
with the
intervention
Outcome
expected
from this
intervention?
Description
of patient
or problem
B e b r i e f a n d s p e c i f i c
28.
SS/EBM/IKA-UDIP-2010
Do all clinicalquestions contain 4
elements of PICO?
No
The C implies in the question - PIO
Does temulawak increase appetite in undernourished
children?
Asking prevalence – PO
How many percent of patients with TIA who subsequently
develop stroke?
29.
SS/EBM/IKA-UDIP-2010
Relevance: Type ofEvidence
POE: Patient-oriented evidence
mortality, morbidity, quality of life
DOE: Disease-oriented evidence
pathophysiology, pharmacology, etiology
30.
SS/EBM/IKA-UDIP-2010
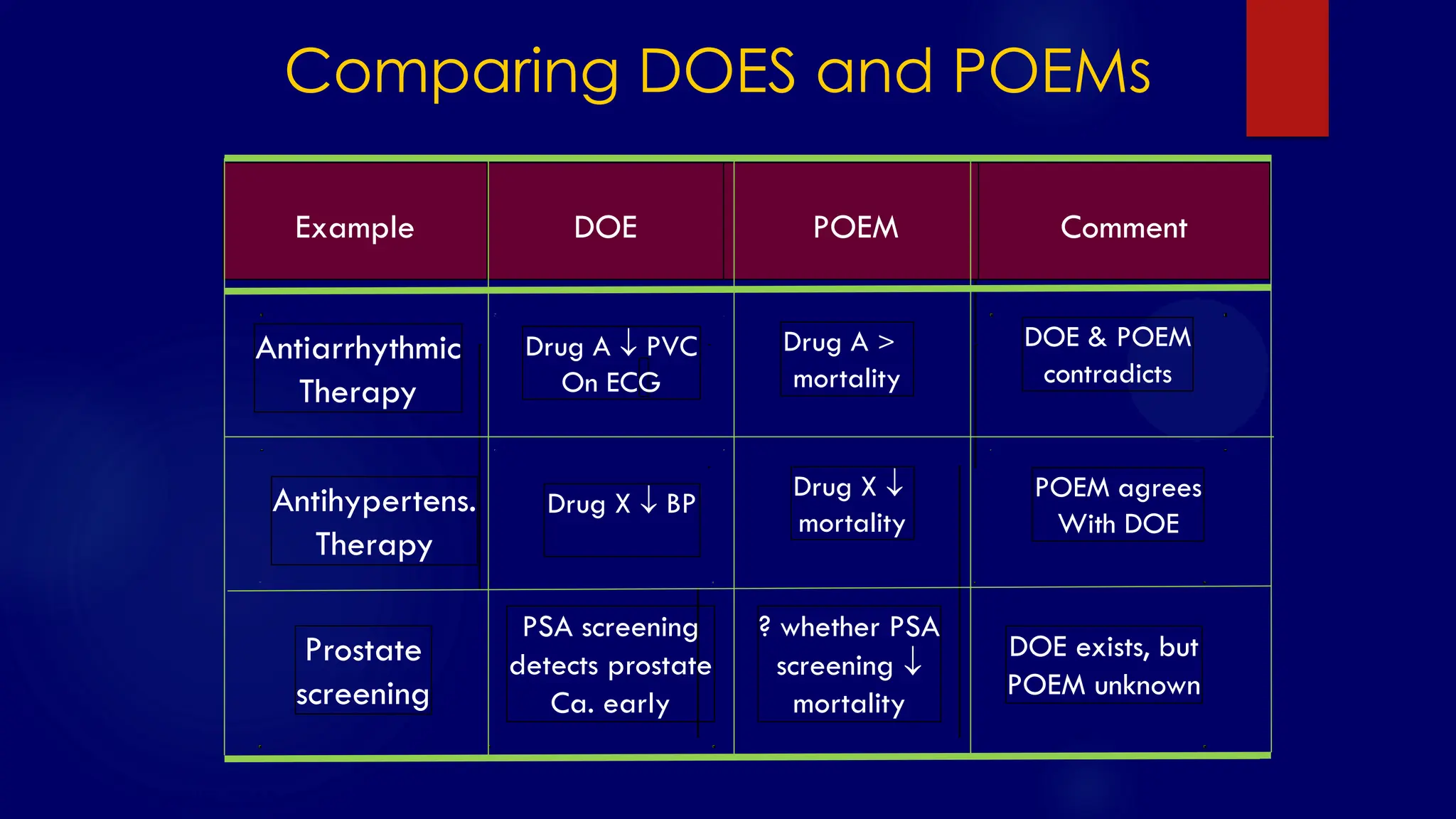
Comparing DOES andPOEMs
Prostate
screening
PSA screening
detects prostate
Ca. early
? whether PSA
screening
mortality
DOE exists, but
POEM unknown
Antiarrhythmic
Therapy
Antihypertens.
Therapy
Drug A PVC
On ECG
Drug X BP
Drug X
mortality
Drug A >
mortality
DOE & POEM
contradicts
POEM agrees
With DOE
Example DOE POEM Comment
SS/EBM/IKA-UDIP-2010
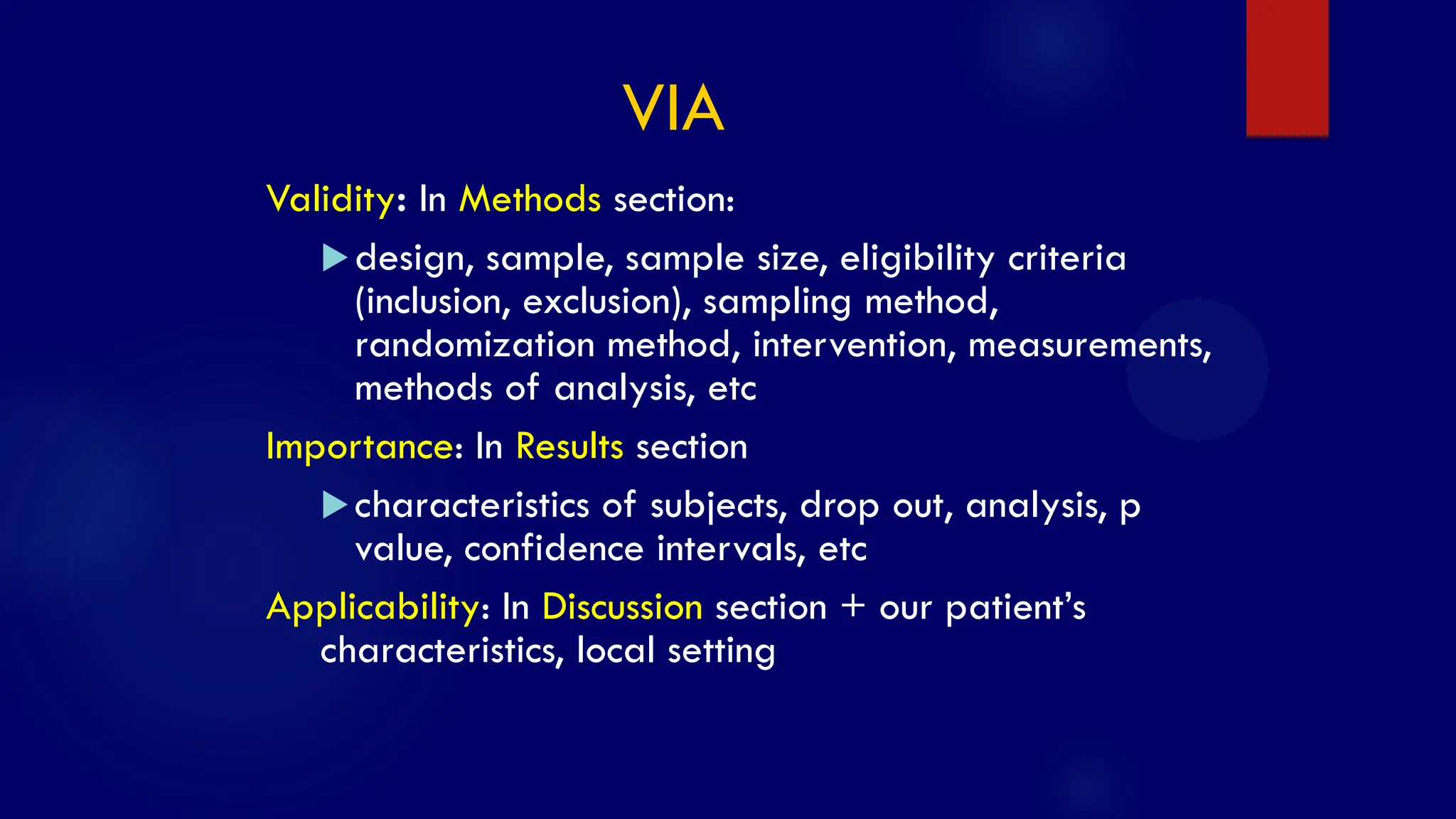
Validity: In Methodssection:
design, sample, sample size, eligibility criteria
(inclusion, exclusion), sampling method,
randomization method, intervention, measurements,
methods of analysis, etc
Importance: In Results section
characteristics of subjects, drop out, analysis, p
value, confidence intervals, etc
Applicability: In Discussion section + our patient‟s
characteristics, local setting
VIA
34.
SS/EBM/IKA-UDIP-2010
Example:
Critical appraisal fortherapy
Were the subjects randomized?
Were all subjects received similar treatment?
Were all relevant outcomes considered?
Were all subjects randomized included in the analysis?
Calculate CER, EER, RRR, ARR, and NNT
Were study subjects similar to our patients in terms of
prognostic factors?
35.
SS/EBM/IKA-UDIP-2010
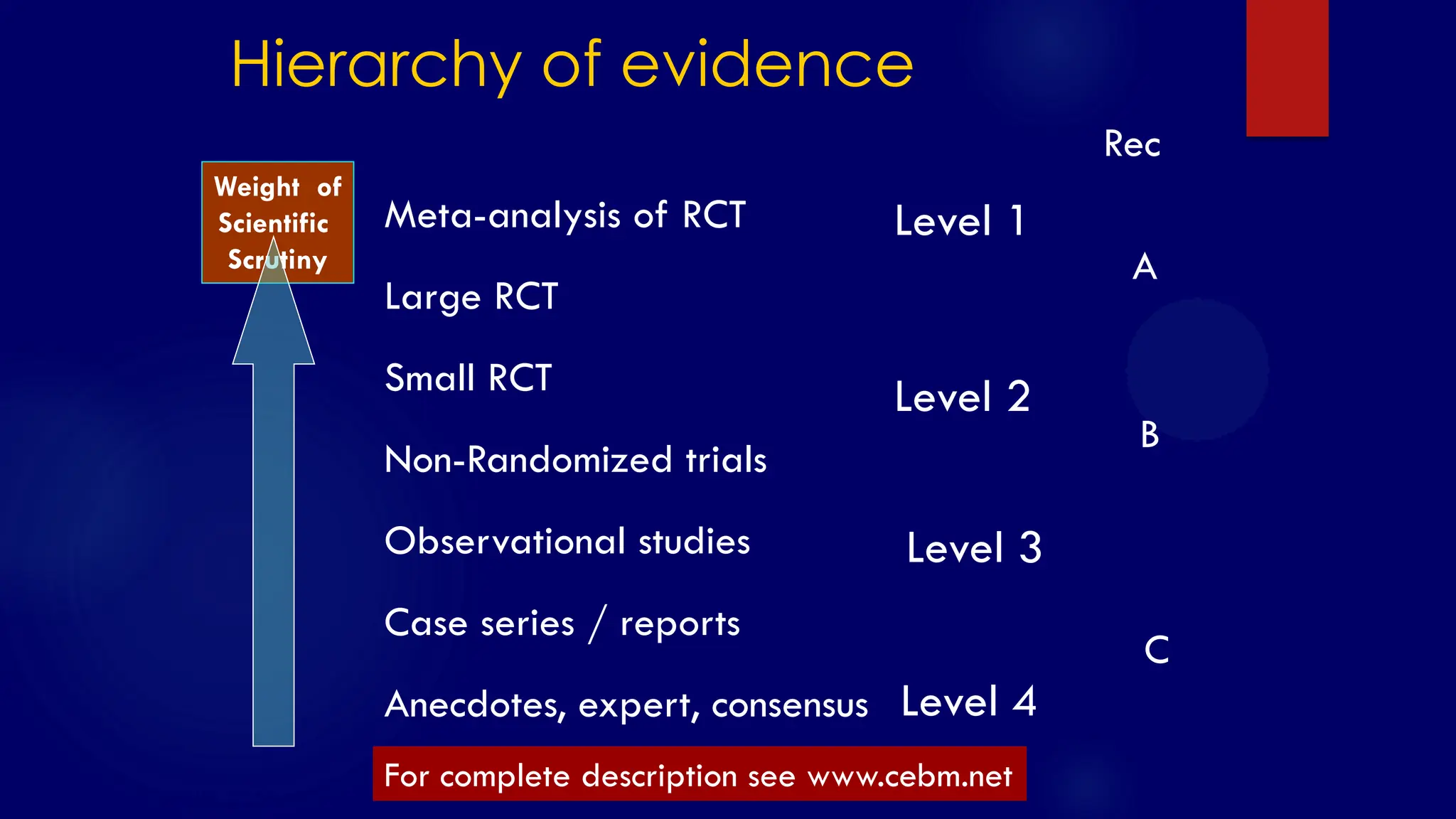
Hierarchy of evidence
Meta-analysisof RCT
Large RCT
Small RCT
Non-Randomized trials
Observational studies
Case series / reports
Anecdotes, expert, consensus
Level 1
Level 2
Level 3
Level 4
A
B
C
Rec
Weight of
Scientific
Scrutiny
For complete description see www.cebm.net
36.
SS/EBM/IKA-UDIP-2010
Implementation of EBMpractice:
How to get started
1. Teaching EBM in medical schools / PPDS
Easier than to change the already existing attitude
Most important
May be included in formal curricula or integrated in
existing activities: ward rounds, on calls, case
presentations, group discussions, journal clubs, etc
2. Workshop for teaching staff
3. Workshop for practitioners, incl. Nurses
37.
SS/EBM/IKA-UDIP-2010
Resistance to EBMteaching
& learning
Rudimentary skill in critical appraisal /
methodological skill
Limited resources, esp. Time factor
Lack of high quality evidence
Skepticism toward evidence-based practice
„Happy‟ with current practice
SS/EBM/IKA-UDIP-2010
EBM makes expensivemedical care
EBM cannot be implemented in developing countries
EBM is costly and time consuming
EBM ignore pathophysiology & reasoning
EBM ignore experience and clinical judgment
EB-guidelines etc interfere with professional autonomy
Criticism to EBM
41.
SS/EBM/IKA-UDIP-2010
Criticism to EBM
EBMmakes expensive medical care: cf
Routine antibiotics for ARTI & diarrhea
Liberal indication for C-section
Unnecessary sophisticated procedures / exams
Unnecessary / harmful treatment: steroid for recurrent
cough
42.
SS/EBM/IKA-UDIP-2010
Criticism to EBM
EBMcannot be implemented in developing countries
By definition EBM is implemented if it is
implementable (patient‟s preference and local
condition) – for the benefit of the patients and the
community
43.
SS/EBM/IKA-UDIP-2010
Criticism to EBM
EBMis costly and time consuming
EBM does requires facilities at the cost of quality
medical care!
Cost benefit ratio should be assessed in individual
and community levels
44.
SS/EBM/IKA-UDIP-2010
Criticism to EBM
EBMignores pathophysiology & reasoning
EBM encourages clinical reasoning in the light of valid and
important evidence
Pathophysiology and reasoning should be seen as hypothesis
and should end-up in empirical evidence
45.
SS/EBM/IKA-UDIP-2010
Criticism to EBM
EBMignore experience and clinical judgment
Personal experience and clinical judgment are by no means can
be eliminated
EBM encourage detailed and systematic documentation of
experience and judgment
EBM encourages clinical reasoning in the light of valid and
important evidence
Subjective experience should be, whenever possible, translated
into more objective measures
46.
SS/EBM/IKA-UDIP-2010
Criticism to EBM
EB-guidelinesinterfere with professional autonomy
Professional conduct (competence, altruism, openness, collegiality,
ethics) is encouraged in EBM
Every physician should develop their own practice attitude based
on his/her profess-ionalism, valid evidence, and patient‟s values
Development of clinical guidelines and other standards of care
should be seen as a guide and implemented according to clinical
setting
47.
SS/EBM/IKA-UDIP-2010
Advantages of EBM
Encouragesreading habit
Improves methodological skill (and willingness to do research?!)
Encourages rational & up to date management of patients
Reduces intuition & judgment in clinical practice, but not eliminates
them
Consistent with ethical and medico-legal aspects of patient
management
48.
SS/EBM/IKA-UDIP-2010
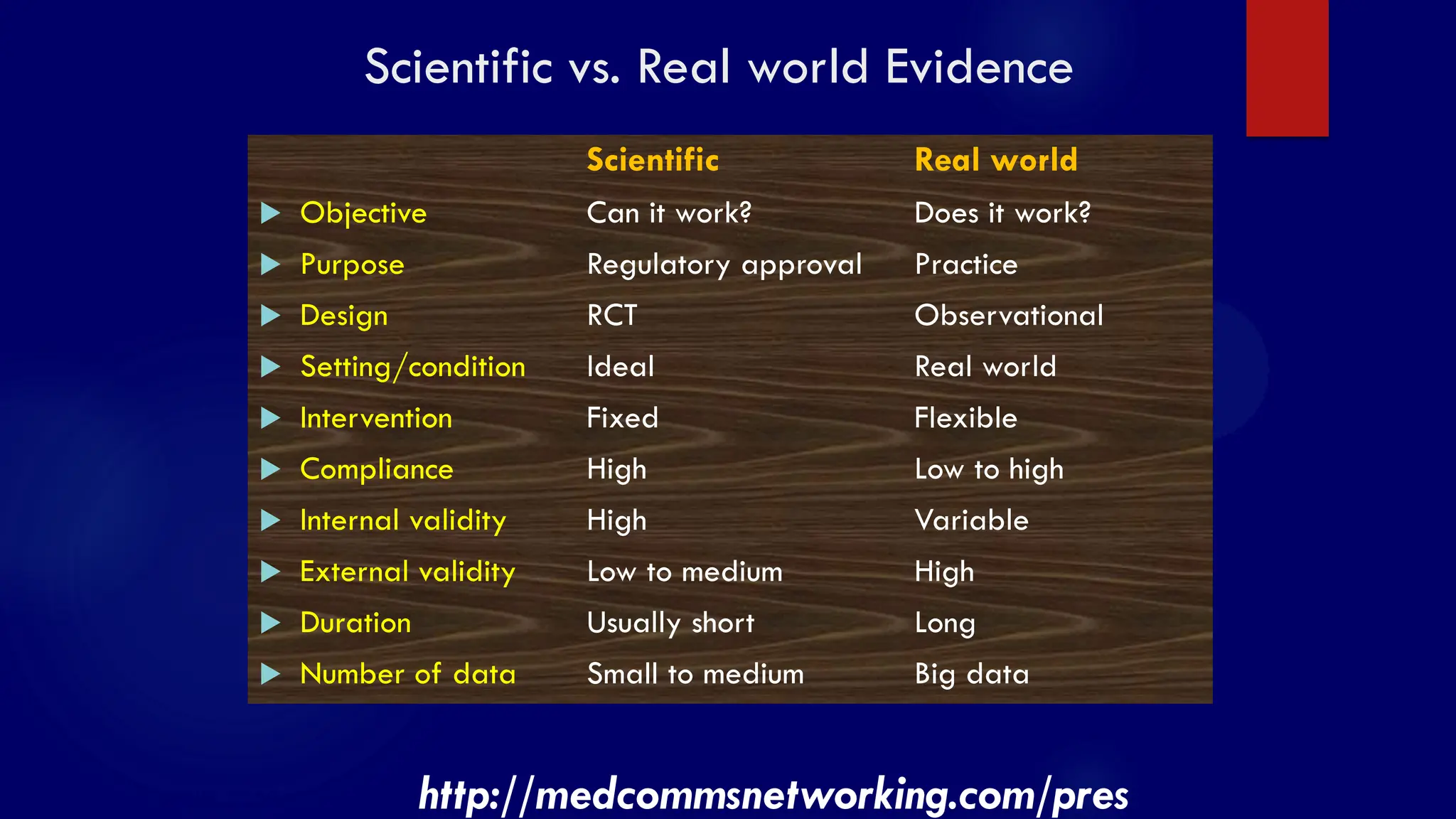
Scientific vs. Realworld Evidence
Scientific Real world
Objective Can it work? Does it work?
Purpose Regulatory approval Practice
Design RCT Observational
Setting/condition Ideal Real world
Intervention Fixed Flexible
Compliance High Low to high
Internal validity High Variable
External validity Low to medium High
Duration Usually short Long
Number of data Small to medium Big data
http://medcommsnetworking.com/pres
49.
SS/EBM/IKA-UDIP-2010
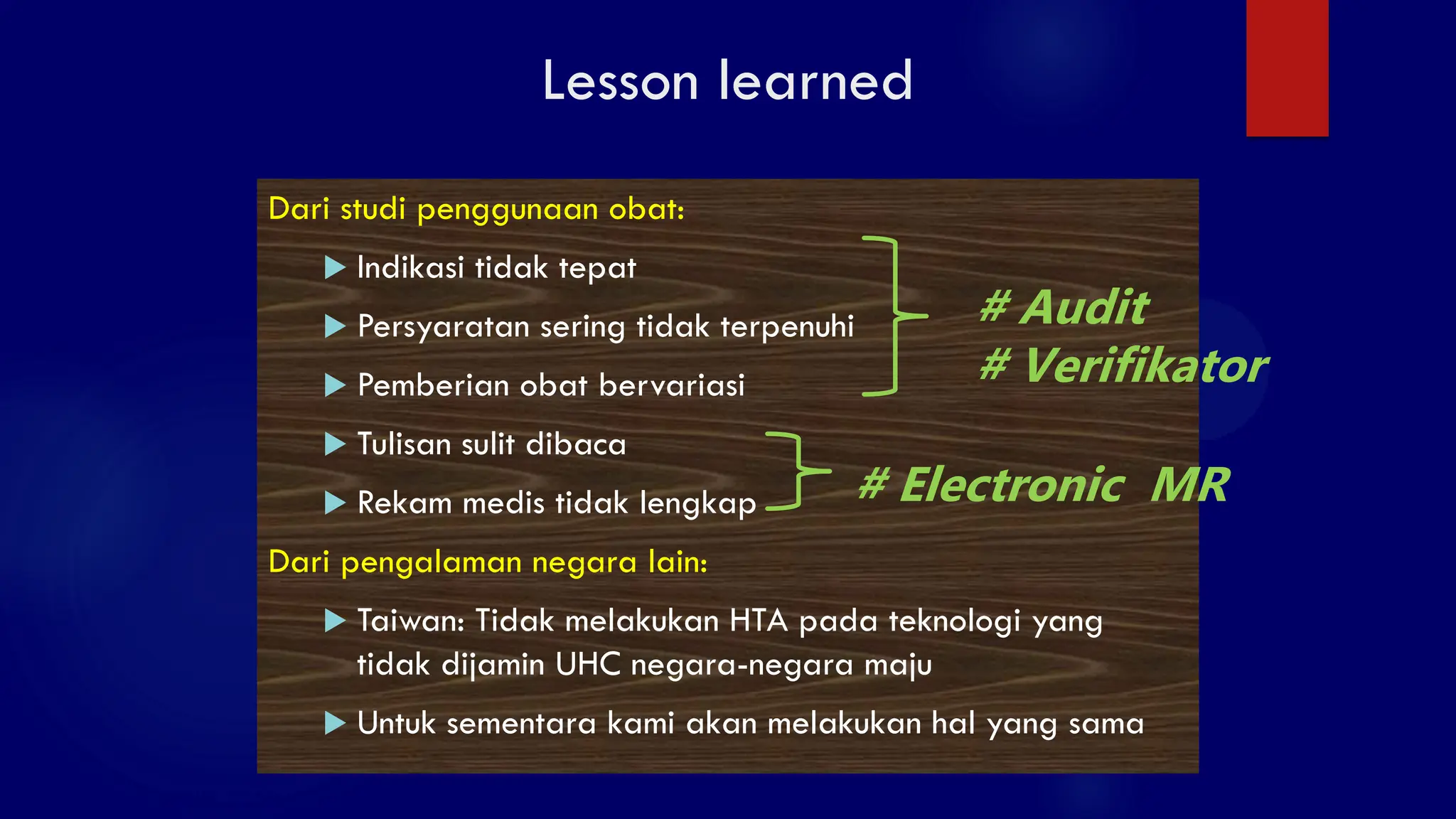
Lesson learned
Dari studipenggunaan obat:
Indikasi tidak tepat
Persyaratan sering tidak terpenuhi
Pemberian obat bervariasi
Tulisan sulit dibaca
Rekam medis tidak lengkap
Dari pengalaman negara lain:
Taiwan: Tidak melakukan HTA pada teknologi yang
tidak dijamin UHC negara-negara maju
Untuk sementara kami akan melakukan hal yang sama
# Audit
# Verifikator
# Electronic MR
SS/EBM/IKA-UDIP-2010
Evidence-based …
Evidenve-based medicine
Evidence-basedcardiology, pediatrics, neurology, etc etc
Evidence-based clinical practice guidelines
Evidence-based clinical audits
Evidence-based health technology assessment
Evidence-based community health development
Evidence-based health policy making
Evidence-based …… anything
52.
SS/EBM/IKA-UDIP-2010
“A 21st centuryclinician who cannot critically
read a study is as unprepared as one who
cannot take a blood pressure or examine the
cardiovascular system.”
BMJ 2008:337:704-705