Downloaded 3,182 times


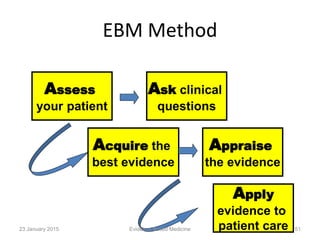
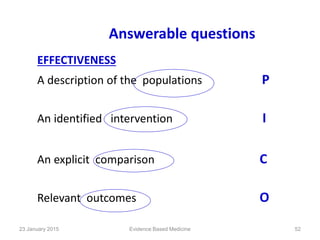
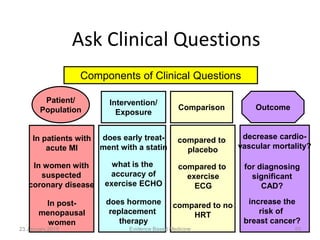
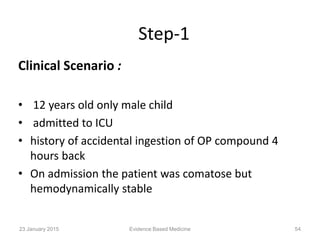
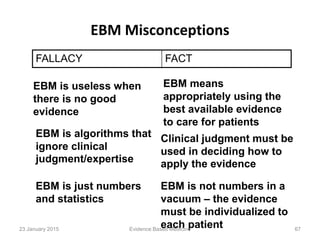
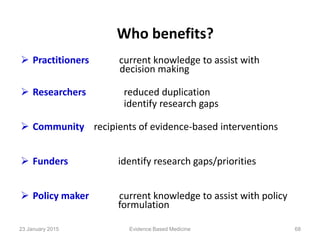
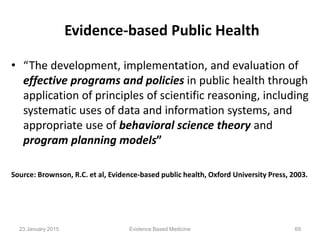
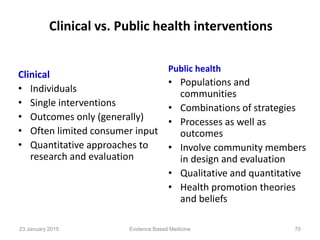



The document is a presentation by Dr. Suhasini K. on evidence-based medicine (EBM), discussing its definition, importance, and the integration of clinical expertise with the best research evidence. It outlines the evolution of EBM, critical appraisal of literature, and a five-step approach to its practice, emphasizing the need for proper decision-making in clinical settings. Additionally, it highlights the misconceptions surrounding EBM and its significance in improving patient care and optimizing clinical practices.

























































































