Downloaded 11 times






![[1.]
Sources for Background Questions :
• Textbooks
• Handbooks
• Manuals
Background
Questions
Acquire](https://image.slidesharecdn.com/ebm-160727183431/85/Ebm-36-320.jpg)



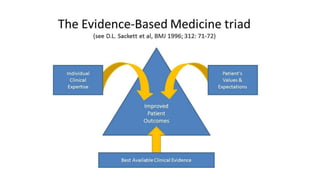
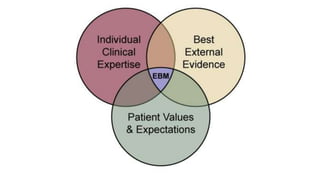
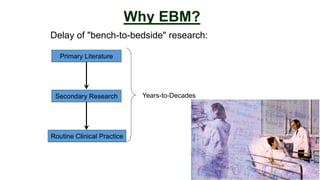
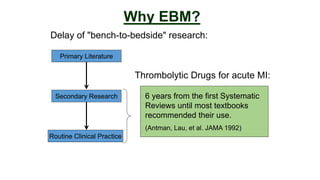
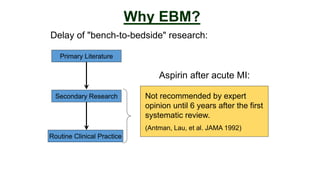
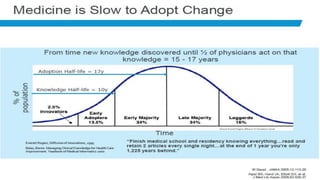
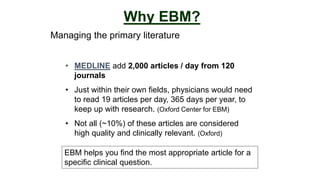
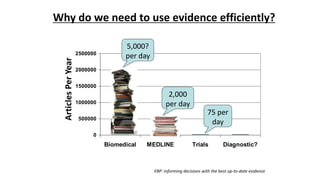
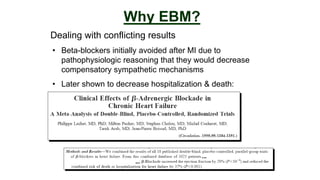
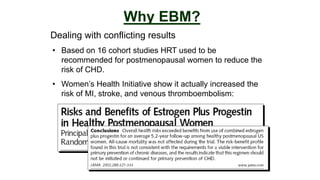
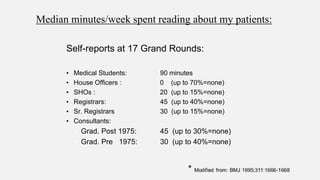
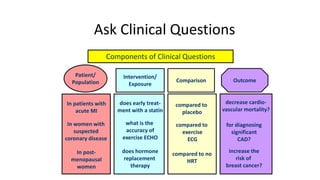
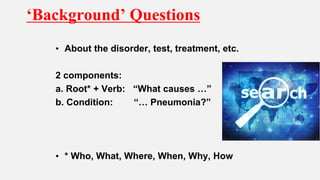
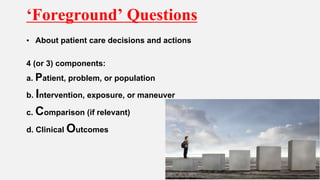
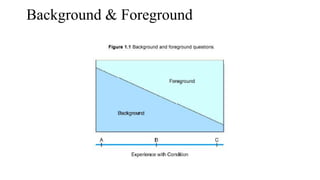
This document discusses evidence-based medicine (EBM), including what it is, why it is needed, and how it works. It notes that EBM is needed to demonstrate treatment effectiveness, utilize cost-effective measures, and deal with conflicting research results. It also helps clinicians efficiently manage the large amount of primary literature being produced each day and counter misleading drug marketing. The document outlines the EBM process, including how to form clinical questions using PICO elements and searching various sources like textbooks, guidelines, and randomized controlled trials to find the best evidence to answer questions.









































































































