
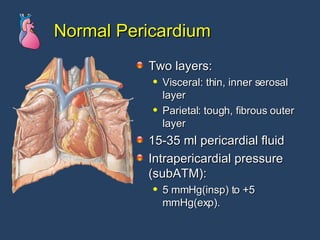


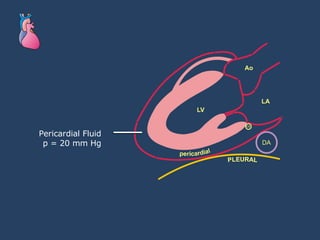
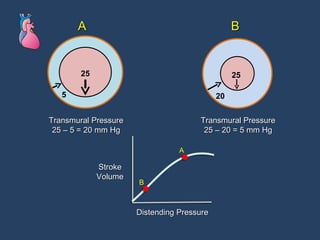
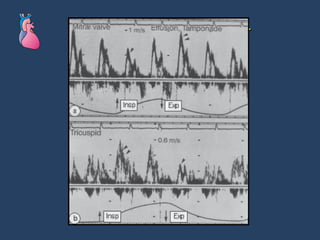
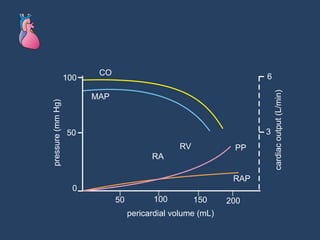
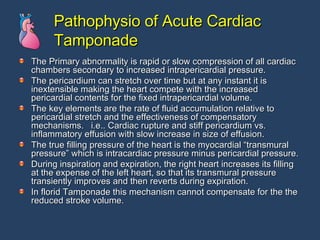

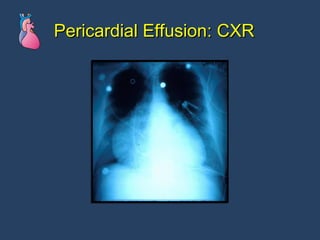
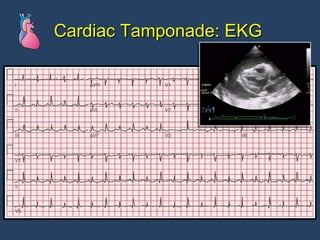
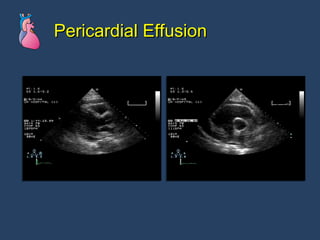
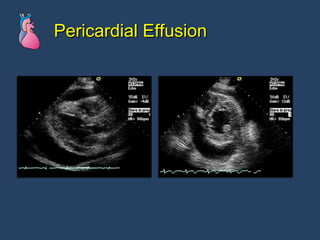
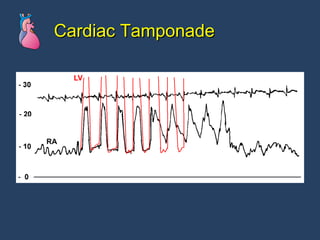
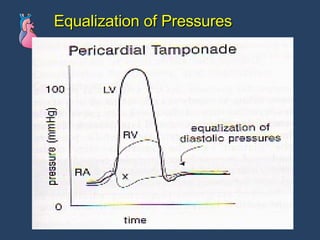
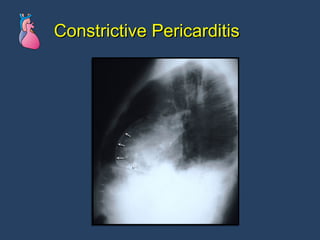
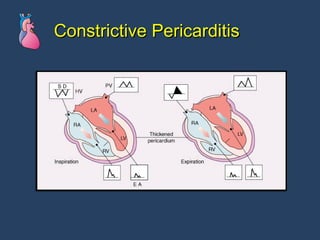
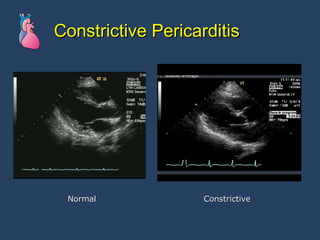
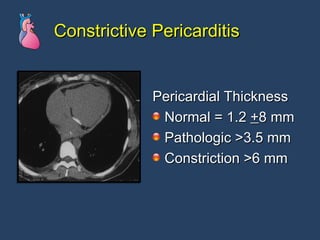
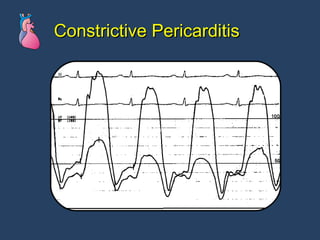
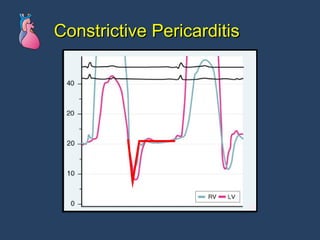
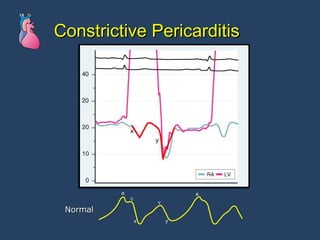
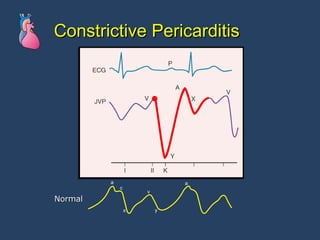
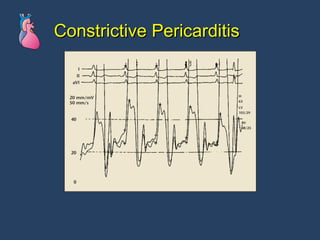
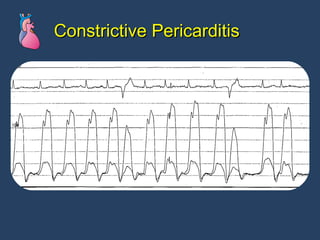
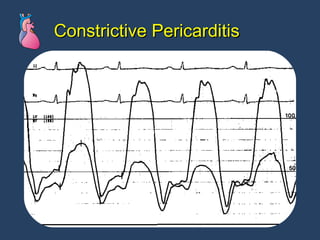
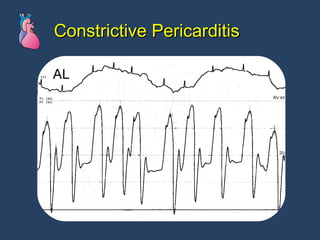
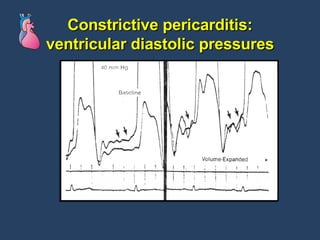
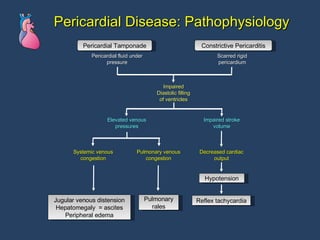

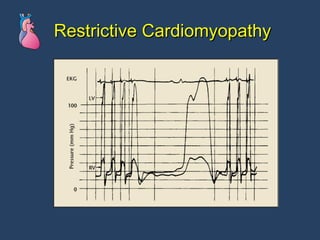

The document discusses various pericardial diseases including normal anatomy, pericarditis, pericardial effusions, cardiac tamponade, and constrictive pericarditis. Key points include: - Pericardial effusions can lead to cardiac tamponade by exerting pressure on the heart and restricting filling. - Cardiac tamponade is diagnosed using echocardiogram, chest x-ray and equalized diastolic pressures on catheterization. - Constrictive pericarditis involves thickened pericardium constraining all chambers and is diagnosed using characteristic hemodynamic tracings on catheterization.























































































