Downloaded 870 times






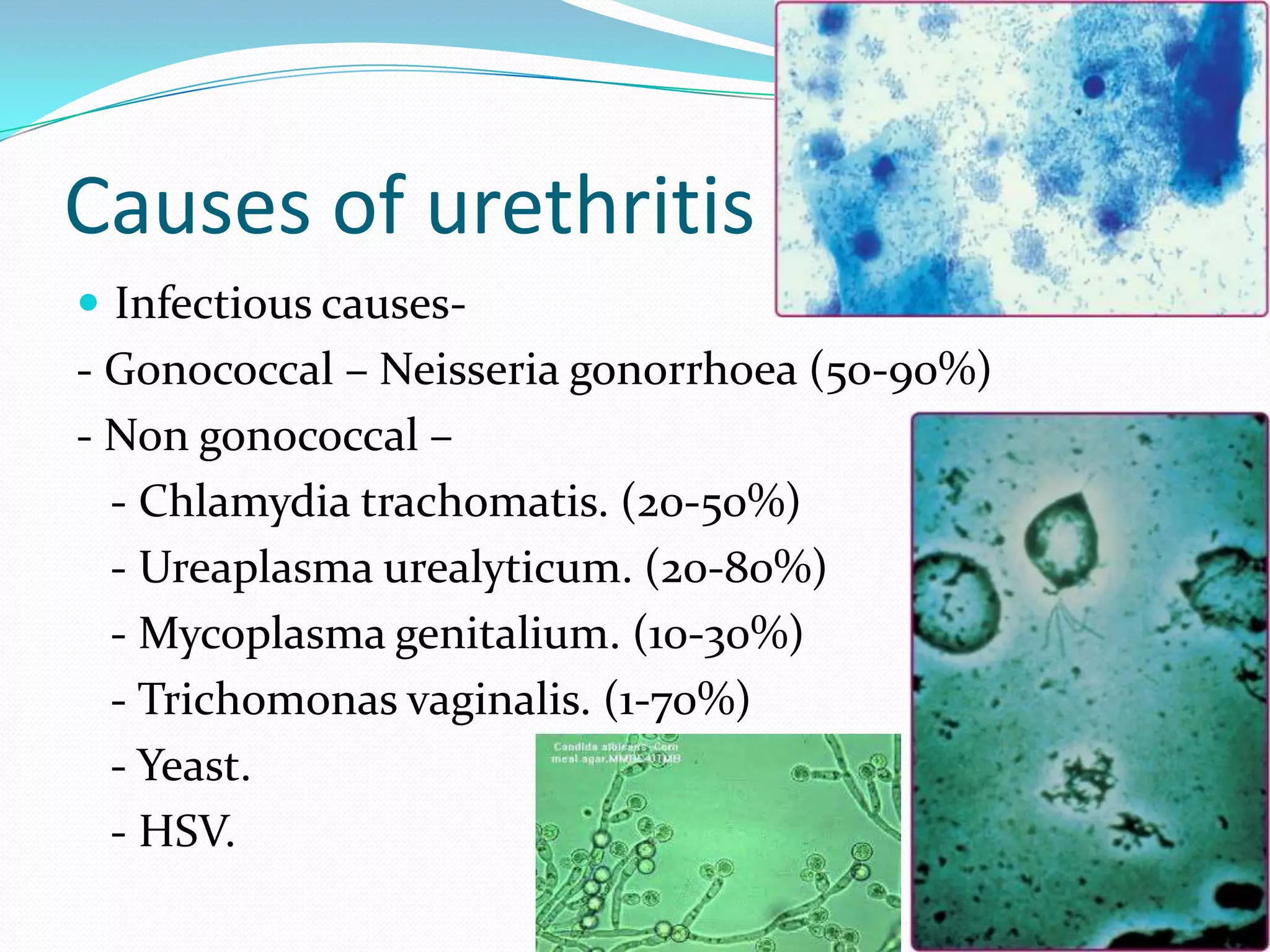














































This document discusses urethritis and its causes. It begins by defining urethritis as inflammation of the urethra, which can cause discharge and dysuria. The main causes of urethritis discussed are infectious agents like Neisseria gonorrhoeae, Chlamydia trachomatis, Ureaplasma urealyticum, and Mycoplasma genitalium. Non-infectious causes like trauma are also mentioned. Gonococcal urethritis and chlamydial urethritis are then described in more detail, outlining their clinical features, diagnosis, treatment and complications. The document concludes with a discussion of the syndromic approach to treating ureth