Downloaded 187 times
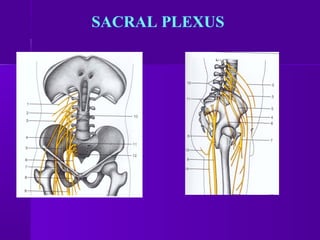

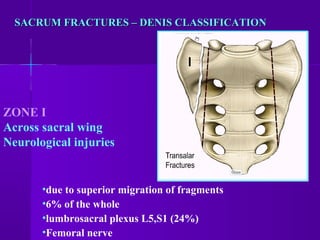

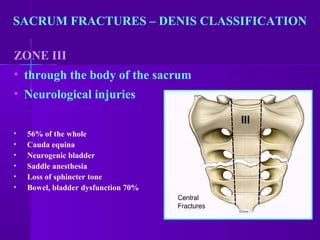
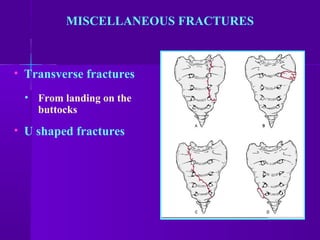

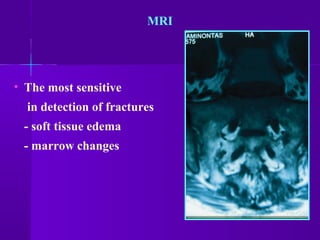
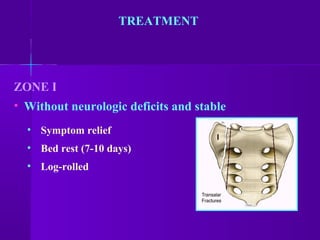
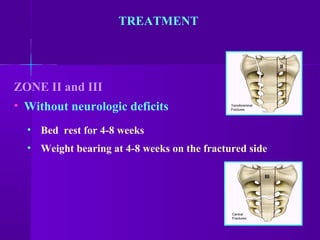

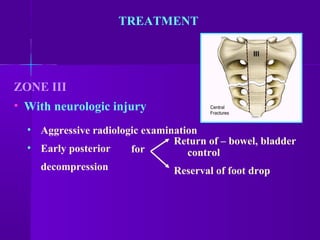

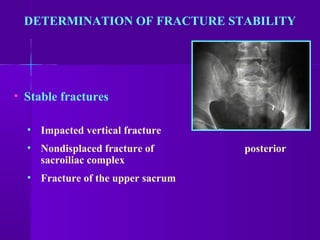
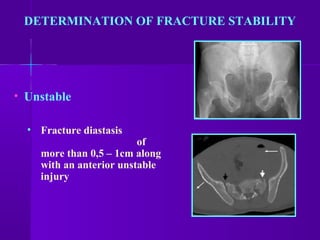


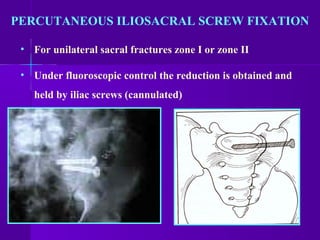
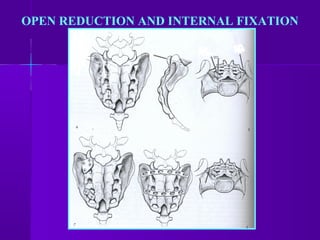




Sacral fractures can result from a blow to the tailbone area from a fall. Women are more commonly affected than men. Physical examination may reveal bruising and tenderness over the sacrum or coccyx. X-rays sometimes do not show fractures if they are minor. More serious fractures are classified by Denis zones, with zone III fractures through the sacral body posing the highest risk of neurological injuries like loss of bladder control. Treatment depends on fracture stability and neurological involvement, ranging from rest and cushioning to sacral laminectomy or open reduction and internal fixation. Coccyx fractures from falls also cause severe pain but generally require only analgesics and cushioning.









































![[Ortho] spine](https://cdn.slidesharecdn.com/ss_thumbnails/orthospine-170307173529-thumbnail.jpg?width=640&height=640&fit=bounds)

































































