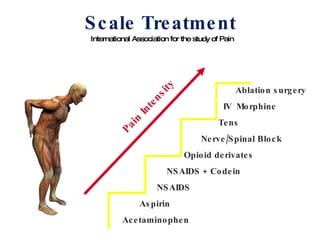
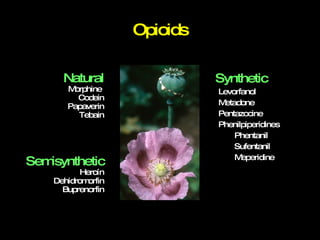
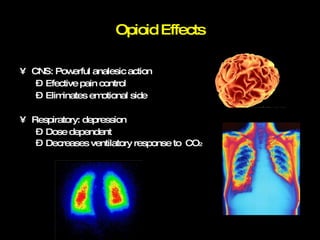
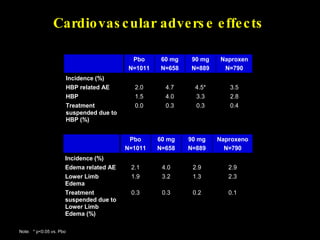
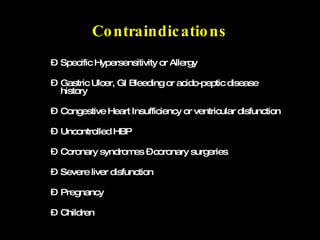
The document discusses the current management of postoperative pain, emphasizing the importance of effective pain management for improving patient quality of life, facilitating faster recovery, and reducing hospital costs. It outlines various pain management techniques, medications (including opioids and NSAIDs), and their respective effects and side effects, along with patient monitoring and assessment protocols. The document also highlights the benefits of cox-2 selective inhibitors like etoricoxib as a promising solution for managing pain with improved safety profiles.














![More Info ? [email_address] chazleal@gmail.com](https://image.slidesharecdn.com/postoppainleal09-090523222909-phpapp01/85/Postoperative-Pain-Management-89-320.jpg)







































































































