Downloaded 35 times




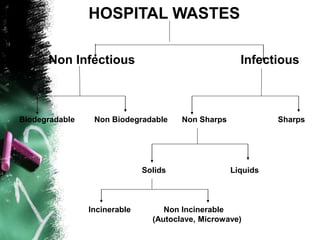
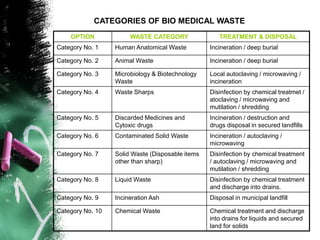
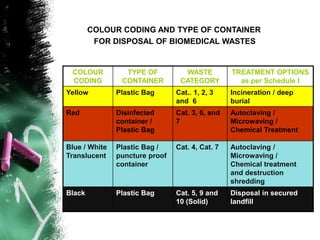






This document discusses waste management, particularly biomedical waste. It begins by defining waste and providing a brief history of waste management. It then outlines various authorities and regulations involved in waste management. It classifies different types of industries and wastes, including domestic, construction, industrial, infectious, and hazardous wastes. The document primarily focuses on proper procedures for handling, segregating, storing, and disposing of biomedical waste to prevent health risks, with a focus on following color-coded systems and treating different categories of waste appropriately. It emphasizes the importance of social responsibility in properly disposing of waste.














































































