Downloaded 144 times


































Gonioscopy is a critical clinical technique for examining the anterior chamber angle, essential for diagnosing and managing glaucoma. It involves either direct or indirect methods, using specialized lenses to overcome reflection issues inherent in standard examinations. While both techniques have advantages and disadvantages, gonioscopy serves various diagnostic and therapeutic purposes related to glaucoma and other anterior segment conditions.
Introduction of the presenter and the topic of Gonioscopy in ophthalmology.
Overview of significant contributors to gonioscopy, including Goldmann (1938) and Barkan's involvement in glaucoma management.
Gonioscopy defined as a technique to examine the anterior chamber angle, crucial for glaucoma diagnosis and therapy planning.
Explanation of how gonioscopy addresses total internal reflection to visualize the anterior chamber angle.
List of conditions for gonioscopy, including angle closure signs, evidence of trauma, diabetes, and other ocular abnormalities.
Classification of gonioscopy into direct and indirect techniques.
Details on direct gonioscopy, including its execution and the use of various direct goniolenses.
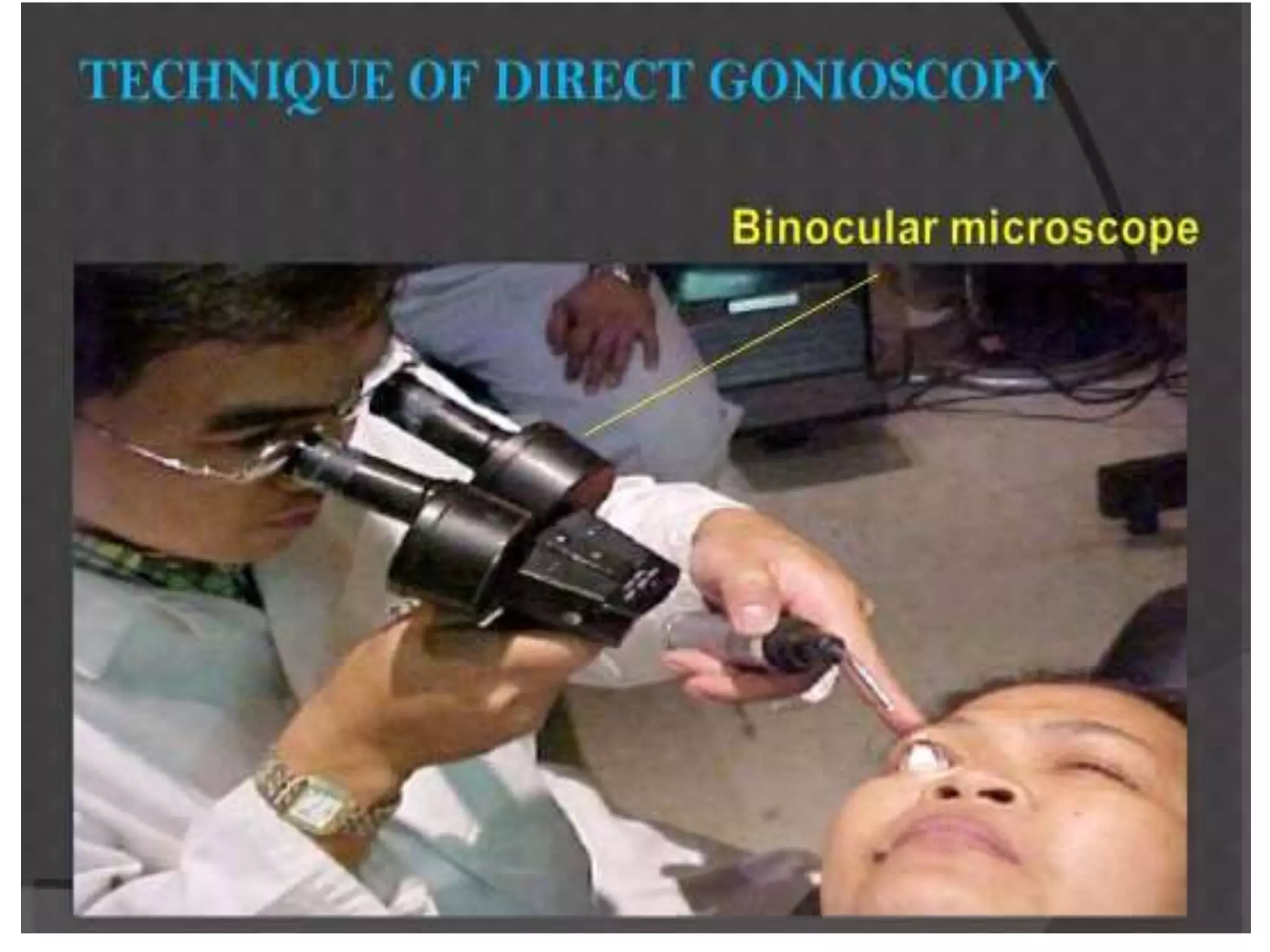
Step-by-step process of performing direct gonioscopy and necessary positioning for optimal viewing.
Key benefits including flexibility, panoramic views, and suitability for various patient positions.
Challenges faced with direct gonioscopy like inconvenience, light reflex issues, and time consumption.
Description of indirect gonioscopy using mirrors or prisms to visualize the anterior chamber angle.
Details on various gonioprisms available for indirect gonioscopy, including advantages and limitations of each type.
Procedure for indirect gonioscopy, including patient and examiner positioning and visualization techniques.
Identifications of key anatomical structures observed in gonioscopy including Schwalbe’s line and others.
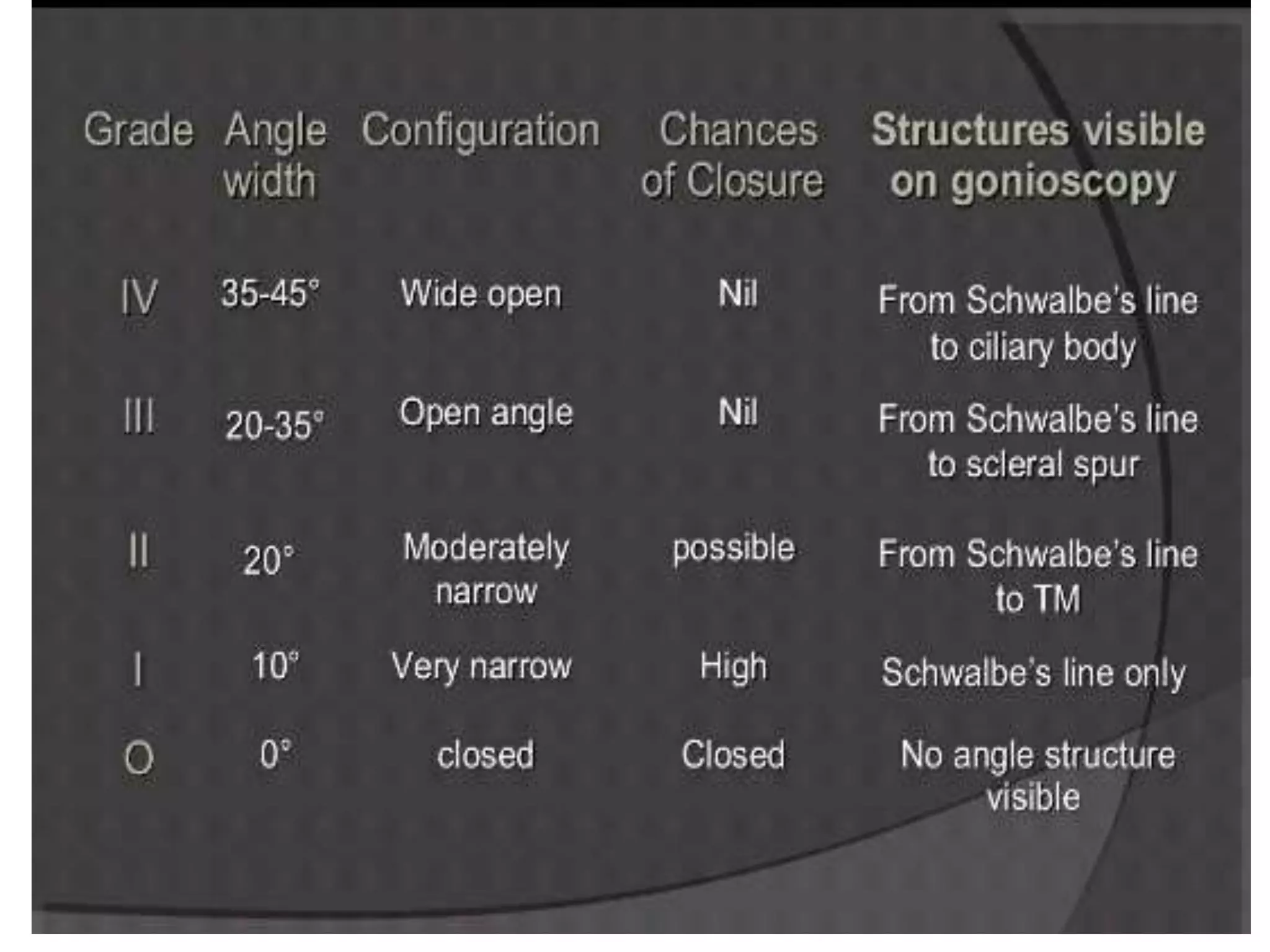
Overview of Scheie’s and Shaffer’s grading systems used for assessing angle width in gonioscopy.
Visual representations and schematic drawings of gonioscopic findings to explain utilized grading.
Diagnostic and therapeutic uses of gonioscopy in various glaucoma types and associated surgical procedures.
Challenges in performing gonioscopy during specific eye conditions and potential complications such as corneal abrasion.
Resources and references used in the presentation, along with closing acknowledgments.



































































