Downloaded 69 times
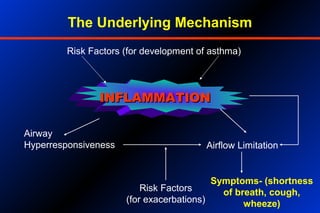
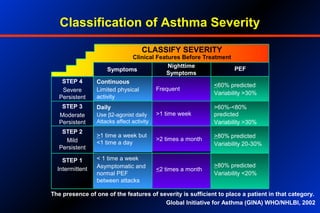

1. Asthma is a chronic inflammatory disorder of the airways that affects 15-20 million people in India. It is characterized by airway hyperresponsiveness and inflammation. 2. Proper diagnosis involves assessing patient history of symptoms, performing a physical exam, and measuring lung function through methods like peak flow meters. Treatment involves a stepwise approach using reliever and preventer medications. 3. Relievers provide quick symptom relief but are not for regular use. Preventers help control inflammation and symptoms over the long-term and include inhaled corticosteroids, long-acting beta-agonists, and other drugs. Combination inhalers containing both a preventer and reliever are often ideal










































![Microsoft+PowerPoint+-+Asthma+4th+year+Lecture+(1)+[Compatibility+Mode].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-230704125445-487a63ed-thumbnail.jpg?width=640&height=640&fit=bounds)

























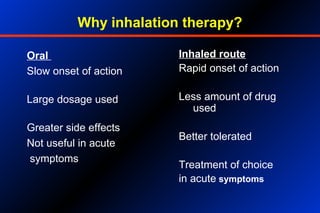
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)