Downloaded 374 times

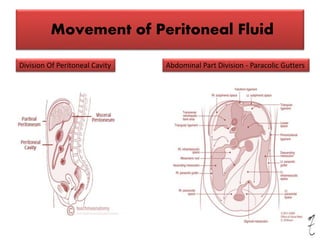
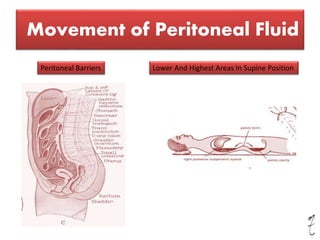

The document presents an extensive overview of the clinical anatomy of the peritoneum, detailing the movement of peritoneal fluid, infections, and conditions such as ascites and internal abdominal hernias. It discusses the roles of structures like the greater omentum in infection localization and surgical applications, as well as the physiology of peritoneal dialysis in renal insufficiency. Clinical symptoms associated with peritoneal pain and diagnostic methods like rebound tenderness are also highlighted.










































































