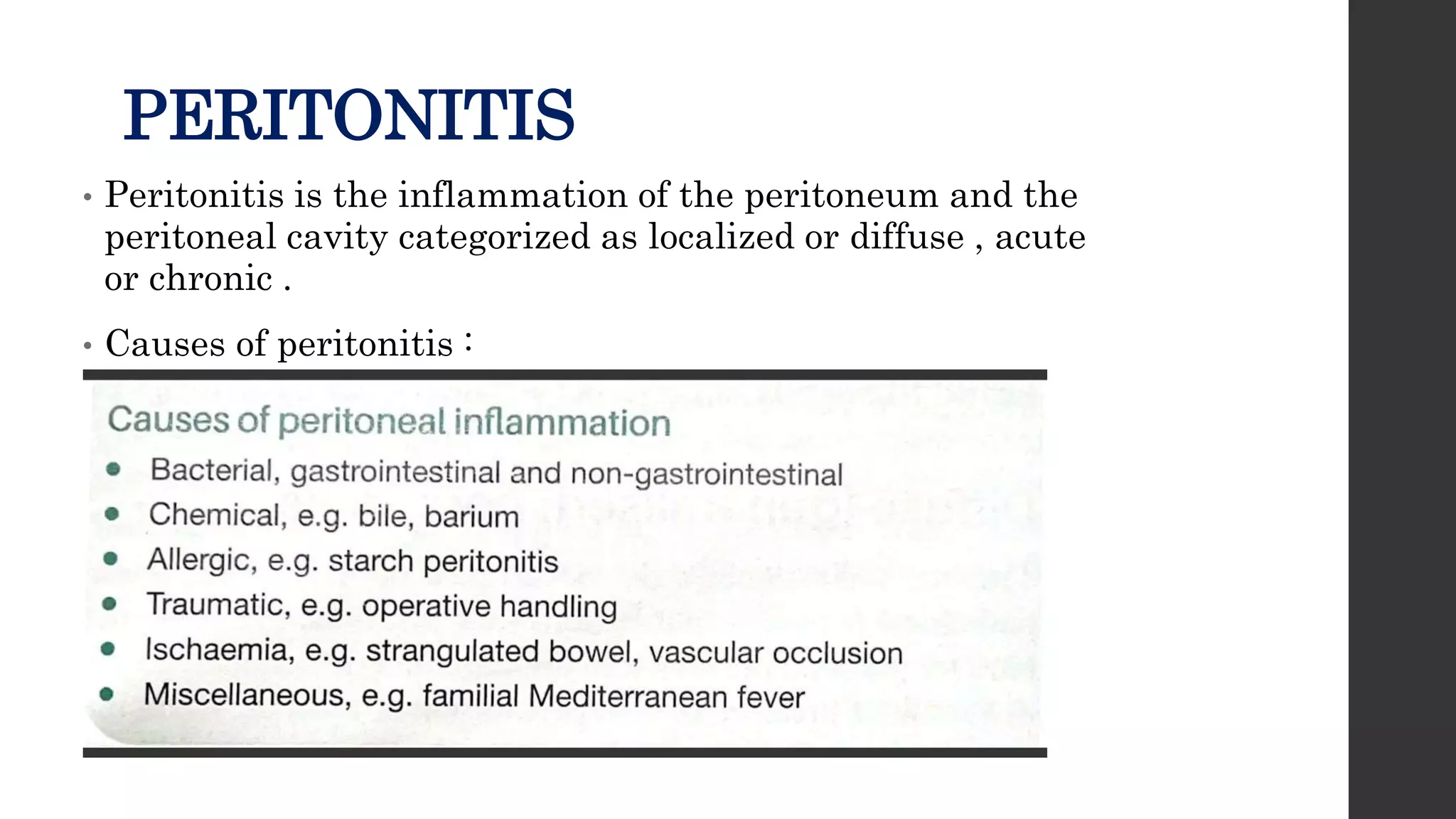
This document discusses peritonitis and intra-abdominal abscesses. It begins by describing the peritoneum, its layers, and peritoneal cavity. Peritonitis is defined as inflammation of the peritoneum and can be localized or diffuse, acute or chronic. Causes include perforation, infection, or surgery. Symptoms include abdominal pain and fever. Treatment involves antibiotics, source control, and drainage if needed. Intra-abdominal abscesses often develop secondary to inflammation and can be identified using imaging. Larger abscesses require drainage by percutaneous or surgical methods.