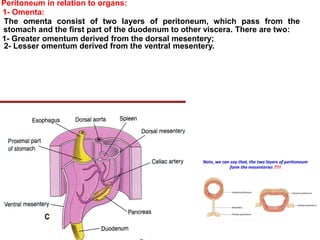
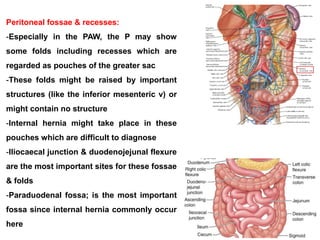
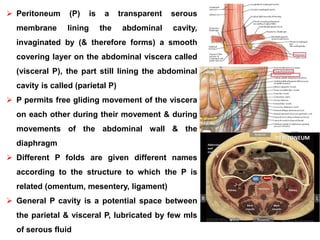
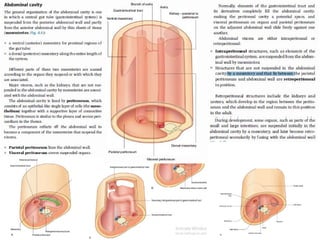
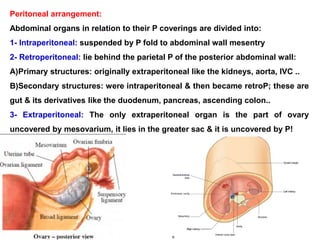
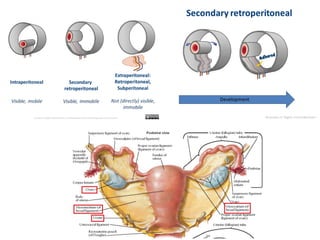
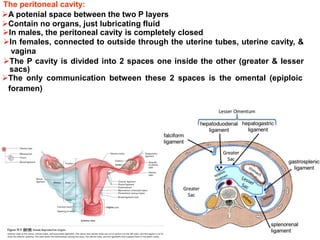
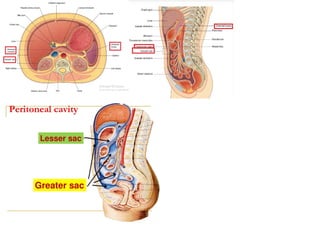
The peritoneum is a serous membrane that lines the abdominal cavity and covers the abdominal organs. It allows the organs to move freely within the cavity. The peritoneum is divided into the parietal peritoneum, which lines the abdominal wall, and the visceral peritoneum, which covers the organs. Different peritoneal folds connect organs to the walls or to other organs, including the omenta, mesentery, mesocolon, and ligaments. The peritoneal cavity is the potential space between the parietal and visceral layers that contains a small amount of fluid. It is divided into the greater and lesser sacs, with the epiploic foramen connecting them.
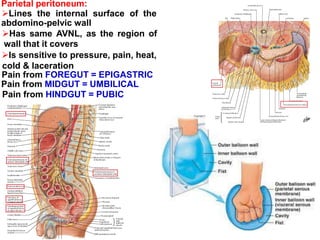
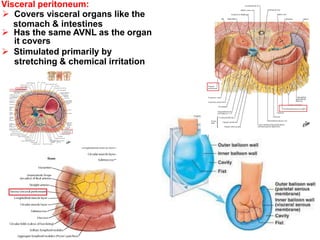
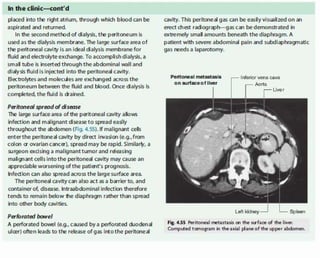
![Ventriculo-peritoneal shunt
The large surface area of the peritoneal cavity is an ideal site of
absorption of CSF if drained to this membrane by a shunt
are commonly used to treat hydrocephalus, the swelling of the brain due to excess buildup of
cerebrospinal fluid (CSF). If left unchecked, the cerebrospinal fluid can build up leading to an
increase in intracranial pressure (ICP) which can lead to intracranial hematoma, cerebral
edema, crushed brain tissue or herniation.[1] The cerebral shunt can be used to alleviate or
prevent these problems in patients who suffer from hydrocephalus or other related diseases.
Shunts can come in a variety of forms but most of them consist of a valve housing connected to
a catheter, the end of which is usually placed in the peritoneal cavity.](https://image.slidesharecdn.com/git3-200520082351/85/peritoneum-17-320.jpg)