Downloaded 32 times
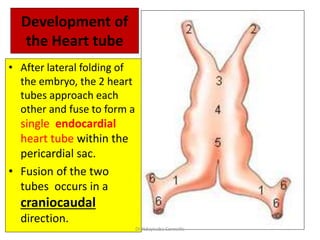

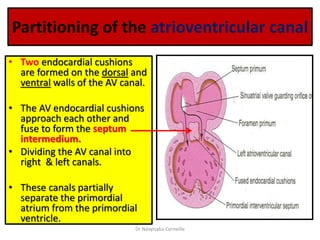
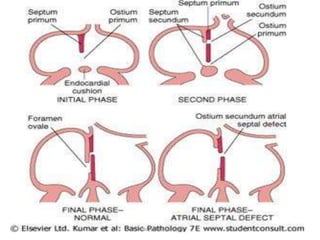
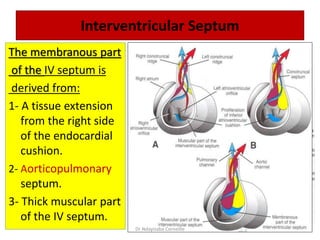
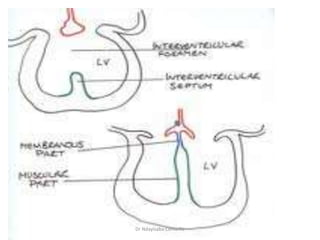
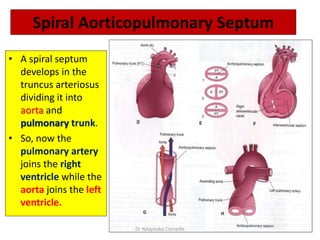
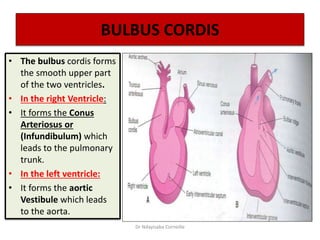
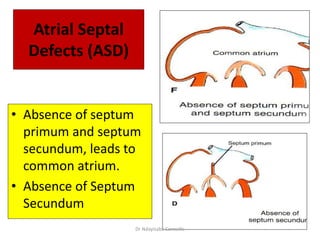
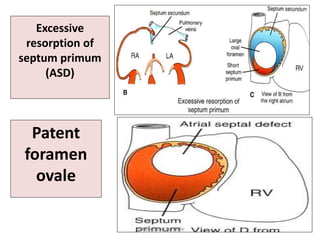
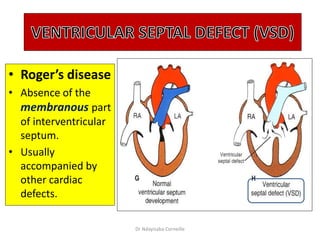
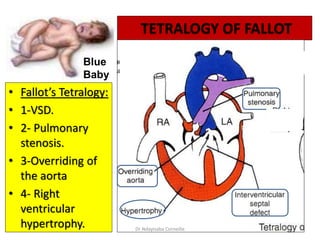
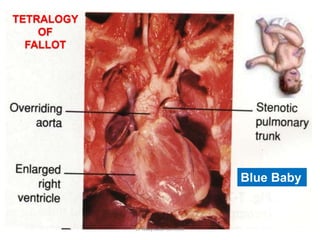
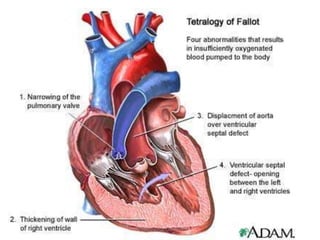

The document discusses the development of the heart and its associated structures, detailing the formation of the heart tube, septa, and ventricular partitioning. It explains the stages of embryonic heart development, including the fusion of heart tubes and common cardiac anomalies such as atrial septal defects and tetralogy of Fallot. The presentation is aimed at providing a comprehensive overview of cardiac anatomy and embryology, highlighting key features and developmental processes.






















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
