Conception and fetal development by Heera KC Parajuli
•Download as PPSX, PDF•
45 likes•8,452 views

Conception and fetal development (Maternal Health)

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Conception and fetal development by Heera KC Parajuli
Similar to Conception and fetal development by Heera KC Parajuli (20)
More from Birat Medical College, Kathmandu University, Nepal
More from Birat Medical College, Kathmandu University, Nepal (17)
Recently uploaded
Recently uploaded (20)
Conception and fetal development by Heera KC Parajuli
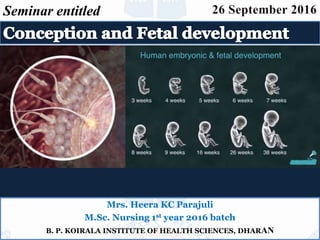
- 1. Mrs. Heera KC Parajuli M.Sc. Nursing 1st year 2016 batch B. P. KOIRALA INSTITUTE OF HEALTH SCIENCES, DHARAN Seminar entitled
- 2. Contents of seminar 10/21/2016 Gametogenesis Ovulation Menstrual cycle Fertilization Fetal development References 2 Prepared by: Heera KC: Conception and fetal development
- 3. GAMETOGENESIS 10/21/2016 Male Female 3 Prepared by: Heera KC: Conception and fetal development Spermatozoon Ovum Maturation process
- 4. GAMETOGENESIS Cont... 10/21/2016 • Both mitosis and meiosis play a role in gametogenesis. • Mitosis provides the precursor cells. • Meiosis brings about the reduction divisions that result in gametes. 4 Prepared by: Heera KC: Conception and fetal development
- 5. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 5 Cell cycle
- 6. 10/21/2016 GAMETOGENESIS 6 Prepared by: Heera KC: Conception and fetal development OOGENESIS GAMETOGENESIS Cont... Oogenesis Spermatogenesis
- 7. 10/21/2016 7Prepared by: Heera KC: Conception and fetal development OOGENESIS Oogenesis The process involved in the development of a mature ovum is called oogenesis.
- 8. Fully matured ovum 10/21/2016 Prepared by: Heera KC: Conception and fetal development 8 Fully mature ovum : largest cell in the body, 130 micron in diameter. Cytoplasm 23 chromosomes(23 x)
- 9. 10/21/2016 9Prepared by: Heera KC: Conception and fetal development Spermatogenesis The process involved in the development of spermatids from the primordial male germ cells and their differentiation into spermatozoa is called spermatogenesis. Primary spermatocytes 16 days. 61 days
- 10. Structure of a mature spermatozoon • It has got two parts, a head and a tail. • The head Condensed nucleus and acrosomal cap. Acrosome is rich in enzymes. • The tail divided into four zones — the neck, the middle piece, the principal piece and the end piece. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 10
- 11. Difference between spermatogenesis and oogenesis. Spermatogenesis differs from oogenesis in three ways 10/21/2016 Prepared by: Heera KC: Conception and fetal development 11 1. All four products of meiosis develop into sperm while only one of the four becomes an egg. 2. Spermatogenesis occurs throughout adolescence and adulthood. 3. Sperm are produced continuously without the prolonged interruptions like in oogenesis.
- 12. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 12
- 13. Ovulation 10/21/2016 Ovulation is a process whereby a secondary oocyte is released from the ovary following rupure 13 Prepared by: Heera KC: Conception and fetal development of a mature Graafian follicle and becomes available for conception. Day 12 Day 1 Day 14Day 20 Day 28
- 14. In each ovarian cycle, Only one secondary oocyte is likely to rupture. It starts at puberty and ends in menopause. 10/21/2016 14 Prepared by: Heera KC: Conception and fetal development Ovulation cont...
- 15. 10/21/2016 15 Prepared by: Heera KC: Conception and fetal development Ovulation cont... Mechanism Changes in follicle Changes in oocyte Preovulatory changes
- 16. • Preovulatory enlargement of the Graafian follicle due to accumulation of follicular fluid. • Measures about 20 mm in diameter. • The cumulus oophorus separates from the rest of the granulosa cells. • The follicular wall near the ovarian surface becomes thinner. Changes in the follicle 10/21/2016 16 Prepared by: Heera KC: Conception and fetal development
- 17. • ovarian cycle 10/21/2016 Prepared by: Heera KC: Conception and fetal development 17 Schematic diagram showing: (A) Mature Graafian follicle on the verge of ovulation (B) Ovulation with discharge of secondary oocyte surrounded by cumulus oophorus (C) Formation of corpus luteum (D) Secondary oocyte after first maturation division with formation of first polar body and (E) Microscopic structure of corpus luteum
- 18. Significant changes occur just prior to ovulation (few hours). Cytoplasmic volume is increased. Completion of the arrested first meiotic division occurs with extrusion of first polar body, each containing haploid number of chromosomes (23, X). Changes in the oocyte 10/21/2016 19 Prepared by: Heera KC: Conception and fetal development
- 19. CAUSES 10/21/2016 20 Prepared by: Heera KC: Conception and fetal development 2.Stretching factor(a passive stretching process of granulosa cells.) Contraction of the micromuscles in the theca externa and ovarian stroma due to increased prostaglandin secretion. Endocrinal •LH surge •FSH rise
- 20. Endocrinal 10/21/2016 21 Prepared by: Heera KC: Conception and fetal development LH surge: Sustained peak level of estrogen for 24–36 hours in the late follicular phase → LH surge occurs from the anterior pituitary. •Ovulation approximately occurs 16–24 hours after the LH surge. •LH peak persists for about 24 hours.
- 21. Endocrinal 10/21/2016 22 Prepared by: Heera KC: Conception and fetal development The LH surge stimulates completion of reduction division of the oocyte and initiates luteinization of the granulosa cells, synthesis of progesterone and prostaglandins FSH rise: Preovulatory rise of progesterone facilitates the positive feedback action of estrogen to induce FSH surge → increase in plasminogen activator → plasminogen → plasmin → helps lysis of the wall of the follicle.
- 22. The follicle is changed into corpus luteum. EFFECT OF OVULATION 10/21/2016 23 Prepared by: Heera KC: Conception and fetal development Menstruation is unrelated with ovulation. The ovum is picked up into the Fallopian tube, and undergoes either degeneration or further maturation,if fertilization is to occur.
- 23. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 24 Reproductive cycle A. Ovarian cycle- B. Anterior pituitary cycle C. Ovarian hormones D. Uterine cycle Proliferative phasephase Secretory phase
- 24. • Fertilization is the process of fusion of the spermatozoon with the mature ovum. • It begins with sperm egg collision and ends with production of a mononucleated single cell called the zygote. Definition 10/21/2016 25 Prepared by: Heera KC: Conception and fetal development
- 25. FERTILIZATION Cont... 10/21/2016 (1) To initiate the embryonic development of the egg and (2) To restore the chromosome number of the species. 26Prepared by: Heera KC: Conception and fetal development Objectives
- 26. FERTILIZATION Cont... 10/21/2016 Almost always, fertilization occurs in the ampullary part of the uterine tube. 27Prepared by: Heera KC: Conception and fetal development Normal site for conception/ Fertilization
- 27. APPROXIMATION OF THE GAMETES • Fertilizable life span of oocyte is 12 to 24 hours and sperm is 48 to 72 hours. • Out of hundreds of millions of sperms deposited in the vagina at single ejaculation, only thousands capacitated spermatozoa enter the uterine tube while only 300–500 reach the ovum. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 28
- 28. APPROXIMATION OF THE GAMETES Tubal transport is facilitated by muscular contraction and aspiration action of the uterine tube. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 29 It takes only few minutes for the sperm to reach the Fallopian tube
- 29. CONTACT AND FUSION OF THE GAMETES • Capacitation • Acrosomal Reaction • Cortical Reaction • Development of zygote 10/21/2016 Prepared by: Heera KC: Conception and fetal development 30
- 30. Capacitation • The process of undertaking in the sperm when inside the female genital tract influenced by the secretions of the uterine tube is known as capacitation. • Sperm must be in the female genital tract 4-6 hours before they can fertilize an ovum. • The sperm undergoes changes in the removal of the glycoprotein coat. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 31
- 31. Acrosomal Reaction • The acrosomal layer of the sperm becomes reactive and releases the enzyme hyaluronidase known as the acrosome reaction . 10/21/2016 Prepared by: Heera KC: Conception and fetal development 32 It disperses the corona radiata (outer layer of ovum) allowing access to the zona pellucida .
- 32. Cortical Reaction 10/21/2016 Prepared by: Heera KC: Conception and fetal development 33 • Penetration of the zona pellucida occurs with the aid of several enzymes processed by the sperm which breaks down the proteins of the zona layer. • Upon penetration a chemical reaction known as the cortical reaction occurs which makes it impermeable to other sperms. The first sperm that reaches the zona pellucida penetrates it.
- 33. • The plasma membrane of the sperm and oocyte fuse. • The oocyte at this stage completes the second meiotic division and becomes mature, the pronuclei has 23 haploid chromosomes. • Male and female pronuclei fuses to form a new nucleus that is a combination of the genetic material from both the sperm and the oocyte diploid cell. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 34 Cortical Reaction
- 34. DEVELOPMENT OF ZYGOTE • The male and female gametes each contribute half the complement of chromosomes to make a total of 46. The new cell is called zygote. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 35
- 35. CONTACT AND FUSION OF THE GAMETES 10/21/2016 Prepared by: Heera KC: Conception and fetal development 36 Schematic diagram showing sequence of changes during fertilization : (A) Sperm (acrosome intact) in between the corona radiata cells → attachment with zona → acrosome reacted sperm penetrating the zona → acrosome reacted sperm in the perivitelline space → incorporated sperm with vesiculating head. (B) Formation of male and female pronuclei with completion of second polar body A B
- 36. Zygote cont... 10/21/2016 Prepared by: Heera KC: Conception and fetal development 37 The zygote, thus formed, contains both the paternal and maternal genetic materials. Sex of the child is determined by the pattern of the sex chromosome supplied by the spermatozoon. If the spermatozoon contains ‘X’ chromosome, a female embryo (46, XX) is formed; if it contains a ‘Y’ chromosome, a male embryo (46, XY) is formed.
- 37. DEVELOPMENT OF ZYGOTE Divided into three periods: –Pre-embryonic period: 1st two weeks after fertilization. –Embryonic period: 2- 8 weeks –Fetal period: 8 weeks to birth. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 38
- 38. PRE-EMBRYONIC PERIOD • This period includes the implantation of the zygote into the endometrium. • The embryo takes about 3 days to travel through the fallopian tube to reach the uterus. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 39
- 39. PRE-EMBRYONIC PERIOD • It takes another 3 days to get implanted, usually in the dorsal wall of the uterus . • Thus embryo is about 1 week old when it gets implanted. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 40
- 40. PRE-EMBRYONIC cont... • Zygote undergoes mitotic division and cellular replication known as cleavage which results in the formation of smaller cells known as blastomers. • During this period a strong membrane of glycoprotein called zona pellucida surrounds the zygote. • The zygote mainly gets nourishment (glycogen) from the goblet cells of the uterine tubes and later the secretory cells of the uterus. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 41
- 41. PRE-EMBRYONIC PERIOD cont... The zygote divides into • 2 cells at day 1, (or 30 hours) • 4 at 2 days, • 8 by 2.5 days, • 16 by 3 days, now known as morula, Resembling a mulberry. (16-64 cell stage) 10/21/2016 Prepared by: Heera KC: Conception and fetal development 42
- 42. • Cells bind tightly together in a process known as compactation. • Next cavitation occurs whereby the outermost cells secrete fluid into the morula and a fluid filled cavity or blastocele appears. • This results in the formation of the blastula or blastocyst comprising 58 cells. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 43 PRE-EMBRYONIC PERIOD cont...
- 43. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 44 Schematic representation of the mitotic division of the zygote resulting in formation of: (A) Two-cell stage; (B) Four-cell stage; (C) Morula and (D) Blastocyst A B C D
- 44. • Development of the morula to the blastocyst, has occurred by day 4. • Blastulation 10/21/2016 Prepared by: Heera KC: Conception and fetal development 45 Blastocyst Trophoblast Placenta chorion Inner cell mass Fetus Amnion Umbilical cord
- 45. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 46 Diagrammatic representation of the events — ovulation, fertilization and implantation: (1) Secondary oocyte extruded at ovulation (2) Secondary oocyte in tube (3) Fertilization with extrusion of second polar body (day 14–16) (4) Formation of zygote (5) Two-cell stage (6) Four-cell stage (7) Early morula (day 17) (8) Late morula (day 18) (9) Early blastocyst stage with disappearance of zona pellucida (day 19–20) (10) Early phase of implantation (day 20–21)
- 46. IMPLANTATION Schematic representation showing interstitial implantation of the blastocyst in stratum compactum of the decidua 10/21/2016 47 Prepared by: Heera KC: Conception and fetal development
- 47. • Embedding of the embryo to the walls of uterus. • Also called as Nidation. • Occurs in the endometrium of the anterior or posterior wall of the body near the fundus on the 6th day which corresponds to the 20th day of a regular menstrual cycle. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 48 IMPLANTATION cont...
- 48. • Implantation occurs through four stages. apposition, adhesion, penetration and invasion. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 49 IMPLANTATION cont... APPOSITION: Occurs through pinopod formation. Pinopods are long finger like projections (microvilli) from the endometrial cell surface. These pinopods absorb the endometrial fluid which is secreted by the endometrial gland cells. This fluid, rich in glycogen and mucin provides nutrition to the blastocyst initially.
- 49. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 50 IMPLANTATION cont... Unless this fluid is absorbed, adhesion phase cannot occur. Adhesion of blastocyst to the endometrium occurs through the adhesion molecules like integrin, selectin and cadherin (glycoproteins). Penetration and invasion occur through the stromal cells in between the glands and is facilitated by the histolytic action of the blastocyst. With increasing lysis of the stromal cells, the blastocyst is burrowed more and more inside the stratum compactum of the decidua.
- 50. THE DECIDUA Endometrium during pregnancy is known as the decidua. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 51 Three layers are found.
- 51. THE DECIDUA 1. The basal layer: Lies immediately above the myometrium. Remains unchanged in itself but regenerates the new endometrium during the puerperium. 2. The functional layer: consists of tortuous glands which are rich in secretions. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 52 It provides a secure anchorage for the placenta and allows it access to nutrition and oxygen, but as soon as the baby is born separation can occur.
- 52. 3.The compact layer: This layer forms the surface of the decidua and is composed of closely packed stroma cells and the neck of the glands. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 53 THE DECIDUA BASAL DECIDUA: underneath the blastocyst. CAPSULAR DECIDUA: that which covers it. PARIETAL DECIDUA: remainder of the decidua (true decidua)
- 53. Functions (1) It provides a good nidus for the implantation of the blastocyst. (2) It supplies nutrition to the early stage of the growing ovum by its rich sources of glycogen and fat. (3) Deeper penetration of the trophoblast is controlled by local peptides, cytokines and integrins. (4) Decidua basalis takes part in the formation of basal plate of the placenta. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 54
- 54. GASTRULATION Embryo Development 10/21/2016 Prepared by: Heera KC: Conception and fetal development 55 1.Outer Syncytiotrophoblast (syncytium): •Layer composed of nuclear protoplasm, capable of breaking down the tissues in the process of embedding. Function: Makes nutrients in maternal blood accessible to the developing embryo. During week 2nd, the trophoblast proliferates and differentiates into layers.
- 55. Gastrulation cont... 2. Inner Cytotrophoblast: A well defined single layer of cells which produce a hormone HCG. This hormone is responsible to inform the corpus luteum that pregnancy has begun. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 56 3. A layer of Mesoderm or the primitive gut: Layer having cells similar to inner cell mass. Simultaneously to implantation, the embryo is developing from the embryoblast.
- 56. Embryoblast differentiate into two layers a. Epiblast : closest to the trophoblast, gives rise to cells of the embryo. Epiblast again gives rise to three layers which are collectively known as the primitive streak at around day 15. b. Hypoblast: closest to the blastocyst cavity. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 57
- 57. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 58 epiblast
- 58. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 59
- 59. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 60
- 60. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 61 Bilaminar disc differentiating into trilaminar disc.(week 3)
- 61. GASTRULA LAYERS DEVELOP 1. The Ectoderm: skin and the nervous system. 2. The Mesoderm: bones, muscles, heart, blood vessels and some visceral organs. 3. The Endoderm: mucous membranes and glands Two cavities appear on either side of the embryonic plate. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 62 INTO…PRIMARY GERM LAYERS
- 62. 10/21/2016 63 Prepared by: Heera KC: Conception and fetal development
- 63. The amniotic cavity Epiblast separates from the trophoblast and forms a cavity that lies on the side of the ectoderm, derives from the ectoderm layer. Filled with fluid, enlarges and folds around the embryo gradually. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 64 2. The yolk sac Cavity that lies on the side of the endoderm and develops from the hypoblast. Provides nourishment for the embryo untill the trophoblast is sufficiently developed to take over.
- 64. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 65 Schematic representation of formation of amniotic cavity, secondary yolk sac, extraembryonic coelom and body stalk: (A) Enlargement of extraembryonic coelomic cavity (B) The amniotic sac enlarges and begins to occupy the extraembryonic coelom (C) The amniotic sac has surrounded the embryo with almost completely obliterating theextraembryonic coelom; formation of body stalk completed
- 65. DEVELOPMENT OF PLACENTA • By the end of 2nd month, trophoblast is charactered by great no. of secondary & tertiary villi. • By four month cytotrophblastic cells & connective tissue disappears, only syncytium & endothelial vessel remains (tertiary villi). 10/21/2016 Prepared by: Heera KC: Conception and fetal development 66
- 66. DEVELOPMENT OF PLACENTA • In early stage, villi covers the entire surface of chorion. • As, the pergnancy advances, villi on embryonic pole continues to grow & expand – chorion frondosum (bushy chorion). • Villi on an embryonic pole degenerate- chorion levae. The fusion of amnion & chorion occurs to form aminochorionic membrane. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 67
- 67. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 68
- 68. Placenta is an organ that connects the developing fetus to the uterine wall to allow 10/21/2016 Prepared by: Heera KC: Conception and fetal development 69 •Nutrient uptake •Waste elimination •Gas exchange via the mother’s blood supply •Hormone production •Formation of a barrier. Function as a fetomaternal organ with 2 components- Fetal placenta Maternal placenta
- 69. THE “PLACENTAL BARRIER” • Sugars, fats and oxygen diffuse from mother’s blood to fetus • Urea and CO2 diffuse from fetus to mother • Maternal antibodies actively transported across placenta – Some resistance to disease (passive immunity) • Most bacteria are blocked • Many viruses can pass including rubella, chickenpox, sometimes HIV 10/21/2016 Prepared by: Heera KC: Conception and fetal development 70
- 70. THE “PLACENTAL BARRIER” • Many drugs and toxins pass including alcohol, heroin, mercury • Placental secretion of hormones –Progesterone and HCG (human chorionic gonadotropin, the hormone tested for pregnancy): maintain the uterus –Estrogens and CRH (corticotropin releasing hormone): promote labor 10/21/2016 Prepared by: Heera KC: Conception and fetal development 71
- 71. 10/21/2016 Prepared by: Heera KC: Conception and fetal development 72
- 72. STAGES OF DEVELOPMENT 10/21/2016 Prepared by: Heera KC: Conception and fetal development 73
- 73. 1 Month • First Trimester At the end of four weeks: • Baby is 1/4 inch in length. 10/21/2016 74Prepared by: Heera KC: Conception and fetal development Placenta (sometimes called "afterbirth") begins to develop. The single fertilized egg is now 10,000 times larger than size at conception Heart, digestive system, backbone and spinal cord begin to form.
- 74. Month 2 10/21/2016 75 Prepared by: Heera KC: Conception and fetal development FirstTrimester At the end of 8 weeks: • Baby is 1-1/8 inches long • Heart is functioning. •Eyes, nose, lips, tongue, ears and teeth are forming • Penis begins to appear in boys. •Baby is moving, although the mother can not yet feel movement. •The limb buds are now clearly arms and legs, while the fingers and toes are still developing.
- 75. Month 3 (FirstTrimester) 10/21/2016 76Prepared by: Heera KC: Conception and fetal development At the end of 12 weeks: Baby is 2 1/2 to 3 inches long (4.4cm) Weight is about 1/2 to 1 ounce. Baby develops recognizable form. Nails start to develop and earlobes, arms, hands, fingers, legs, feet and toes are fully formed. Eyes are almost fully developed . Baby's heart rate can be heard at 10 weeks with a special instrument called a Doppler. Baby has developed most of his/her organs and tissues .
- 76. Month 4 10/21/2016 77 Prepared by: Heera KC: Conception and fetal development At the end of 4 months: • Baby is 6 1/2 to 7 inches long • Weight is about 6 to 7 ounces Developing reflexes, such as sucking and swallowing. may begin sucking his/her thumb .Tooth buds are developing. Eyes blink. Sweat glands are forming on palms and soles, well defined Fingers and toes . Sex is identifiable . Bright pink, transparent skin covered with soft, downy hair . Although recognizably human in appearance, the baby would not be able to survive outside the mother's body. Second Trimester
- 77. • Baby is 8 to 10 inches long (13.2 cm) • Weight is about 1 pound. 10/21/2016 78Prepared by: Heera KC: Conception and fetal development At the end of 5 months •Hair begins to grow on baby's head. Soft woolly hair called lanugo will cover its body. Some may remain until a week after birth, when it is shed. •Mother begins to feel fetal movement. • •Internal organs are maturing. •Eyebrows, eyelids and eyelashes appear.
- 78. At the end of 6 months • Baby is 11 to 14 inches long. • Weight is about 1 3/4 to 2 pounds . • Eyelids begin to part and eyes open sometimes for short periods of time. • Skin is covered with protective coating called vernix . • Baby is able to hiccup. 10/21/2016 79Prepared by: Heera KC: Conception and fetal development Month 6 •The baby's inner ear canals are developed at 24 weeks, so researchers speculate the baby can sense its position in the uterus.
- 79. 10/21/2016 80Prepared by: Heera KC: Conception and fetal development Month 7 • Third Trimester At the end of 7 months: • 14 to 16 inches long. • 2 1/2 to 3 1/2 pounds • Taste buds developed . • Fat layers are forming. • Organs are maturing . •Skin still wrinkled and red. • If born at this time, baby will be considered a premature baby and require special care.
- 80. 10/21/2016 81Prepared by: Heera KC: Conception and fetal development Month 8 (Third Trimester) At the end of 8 months: • 16 1/2 to 18 inches long • 4 to 6 pounds weight. • Overall growth is rapid this month . • Tremendous brain growth occurs at this time . • Most body organs are now developed with the exception of the lungs •Movements or "kicks" are strong enough to be visible from the outside . •Kidneys are mature . •Skin is less wrinkled. •Fingernails now extend beyond fingertips.
- 81. Third Trimester At the end of 9 months: • Baby is 19 to 20 inches long • Weight is about 7 to 7 1/2 pounds • The lungs are mature 10/21/2016 82 Prepared by: Heera KC: Conception and fetal development Month 9 Baby is now fully developed and can survive outside the mother's body . Skin is pink and smooth Baby settles down lower in the abdomen in preparation for birth and may seem less active
- 82. FETAL MEMBRANES • Amnion Smooth, tough, translucent membrane derived from inner cell mass. Have role in the formation of amniotic fluid . • Chorion Thick, opaque, friable membrane, derived from trophoblast. Continuous with the chorionic plate which forms the base of the placenta. 10/21/2016 83Prepared by: Heera KC: Conception and fetal development
- 83. REFERENCES • Dutta D.C. Text book of gynaecology,calcutta 8th edition : New Central Agency. 2005. P. 74-89 • Bennett Ruth V., Brown Linda K. Myles text book of midwives. 13th edition. Harcourt Publishers; Churchill Livingstone. 1999. P. 963-979 • Bijlani RL. Understanding medical physiology: a text book for medical students. Third edition. New Delhi; Emca house, Jaypee Brothers Medical Publishers Pvt. Ltd. P . 577-583 • Leifer G. Introduction to maternity and pediatric nursing. Sixth edition.USA: Elsevier Inc; Elsevier Saunders. 2011. P. 31-41 • Pillitteri Adele. Maternal and child health nursing. Fourth edition. Quebecor Versailles prints: Lippincott William Wilkins. 2003. P.67 – 84 • Internet citation on title embryology (cited date:27/september 2016) http://www.medicinenet.com/fetal_development_pictures_slideshow/article.htm l 10/21/2016 84 Prepared by: Heera KC: Conception and fetal development
- 84. 10/21/2016 85 Prepared by: Heera KC: Conception and fetal development Thank you
Editor's Notes
- The process involved in the maturation of two highly specialized cells , spermatozoon in male and ovum in female before they unite to form zygote is called GAMETOGENESIS
- Two new genetically identical daughter cells.(46 chromosomes) By half and 4 gamate cells.
- Replication : capable of division/copying/duplicating genetic material and dividing into two. Four daughter cells. All differ from parents cells and with each other. Genetic diversity and uniqueness with each other.
- Maturation: reduction in half. Cytoplasm.
- anovular menstruation is quite common during adolescence, following childbirth and in women approaching menopause.
- maturation of follicles and development of corpus luteum. LH and FSH levels. estrogen and progesterone Menstrual, proliferative and secretory Series of events ocuring regularly in female.
- ovum, immediately following ovulation is picked up by the tubal fimbriae which partly envelope the ovary, especially at the time of ovulation
- ovum, immediately following ovulation is picked up by the tubal fimbriae which partly envelope the ovary, especially at the time of ovulation
- Mitotic division. Binary division.
- Basal decidua/serotina.- contact with base of decidua.
- Gastrulation is a phase early in the embryonic development of most animals, during which the single-layered blastula is reorganized into a trilaminar ("three-layered") structure known as the gastrula. These three germ layers are known as the ectoderm, mesoderm, and endoderm.
- The yolk sac becomes partly incorporated into the embryo to form the gut. The part that remains outside is incorporated into the body stalk
- A home pregnancy test should be positive at this stage of development (most tests claim positive results one week after a missed period).