2. INTRODUCTION
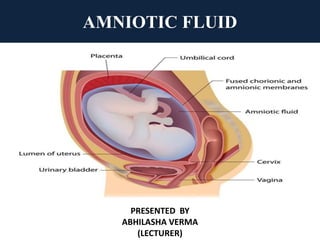
It is clear, yellowish fluid that surrounds and protect fetus in
uterus during pregnancy.
It is also known as liquor amnii.
It is present in amniotic sac.
ORIGIN- Mixed maternal and fetal origin
VOLUME- Volume related to gestational age
At 12 week= 50 ml
At 20 week= 400 ml
At 36 – 38 week= 1000 ml ( Peak)
At term= 600 ml- 800 ml
At 43 week= 200 ml
3. CIRCULATION
• Water in amniotic fluid is completely changed and replaced
every 3 hours.
• Presence of lanugo and epithelium scales in muconium shows
that fluid swallowed by fetus.
• Alkaline, specific gravity is low and hypotonic to maternal
serum at term.
COLOUR- In early pregnancy it is colourless, but near term it
becomes pale straw colored due to presence of exfoliated
lanugo and epidermal cells from fetal skin. It may look turbid
due to presence of vernix caseosa.
PHYSICAL FEATURES
4. • Water = 98-99%
• Solid = 1-2 % ( organic, inorganic & suspended particle)
ORGANIC – Protein ( 0.3%), glucose(20mg%),urea(30 mg%),
NPN(30 mg%), uric acid(4 mg%), Creatinine(2mg%), total lipids(
50%), Hormones(prolectin, insulin and renin)
INORGANIC – Na, Cl, K
SUSPENDED PARTICLE- Lanugo, exfoliated epithelium cell,
vernix ceaseosa, cast off amniotic cell, cells from respiratory
tract, bladder of fetus.
COMPOSITION
5. DURING PREGNANCY
Acts as shock absorber, protecting the fetus from extraneous
injury.
Maintenance of optimum temperature.
Fluid distends the amniotic sac and thereby allow free
movement and growth to fetus.
It prevent adhesion between fetal parts and amniotic sac.
Water supply to fetus.
It permit fetal swallowing essential for GIT development.
FUNCTION
6. DURING LABOR
• Amnion and chorion are combined to form a hydrostatic
wedge which help in dilation of cervix.
• During uterine contraction, it maintain membrane intact.
• It guard against umbilical cord compression and protect the
fetus from trauma.
• It flushes birth canal at end of first stage of labor.
• It protects fetus and prevents ascending infection to uterine
cavity by bactericidal and ascending action.
7. CLINICAL IMPORTANCE
1. Screening for fetal malformation.(serum alpha
fetoprotein)
2. Assessment of fetal wellbeing( Amniotic fluid index)
3. Assessment of fetal lung maturaity( L/S ratio)
4. Diagnosis and follow up of labor.
• Both maternal and fetal sources-
– Maternal vessels in decidua.
– Fetal vessels in placenta
– Amnion and umbilical cord.
– Fetal urine also contribution to volume from 10th
SOURCES
8. PATHWAY EFFECT ON VOLUME DAILY VOLUME ( mL)
Fetal urination Production 1000
Fetal swallowing Resorption 750
Fetal lung fluid secretion Production 350
Intramembranous flow
across fetal vessels on the
placental surface
Resorption 400
Transmembraneous flow
across amniotic membrane
Resorption Minimal
AMNIOTIC FLUID REGULATION
9. AMNIOTIC FLUID ANALYSIS
Imporance of Amniotic Fluid Index-
• Determination of fetal lung maturity
• Detection of fetal distress
• Cytogenic analysis
• Detection of teratology, infection.
• Dectection of heriditory disorder.
• Determination of fetal age.
10. • It is most commonly used method for amniotic fluid volume
assessment.
• Uterus divided into four equal quadrant- right, left, upper, lower
quadrant .
• AFI is the sum of the single deepest pocket from each quardrant.
• Single deepest pocket measurement:-
the ultra sound transducer is held perpendicular to the floor and
parallel to the long axis of the pregnant woman.
• The AFI is the sum of the single deepest pocket from each
quadrant.
• A fluid pocket may contain fetal parts or umbilical cord loops, but
these are not included in measurement.
• Color Doppler is generally used to verify that no umbilical cord is
included in the measurement.
AMNIOTIC FLUID INDEX ( AFI)
11. ABNORMAL COLOR OF AMNIOTIC FLUID
1. Green – muconium stained.
2. Golden- Rh incompatibility & excess haemolysis
3. Saffron ( greenish – yellow)- Postmaturity.
4. Dark colored- concealed haemorrhage
5. Dark brown- IUFD