Downloaded 360 times
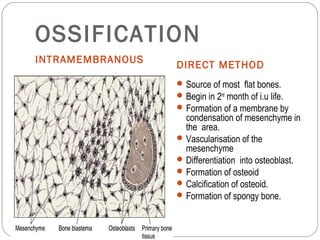

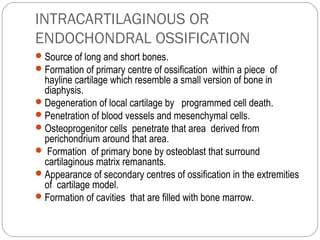

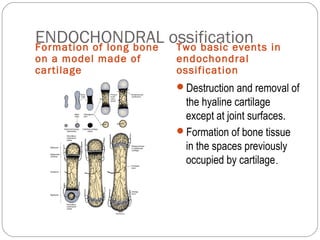

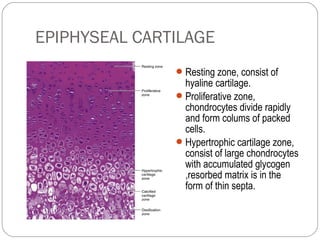
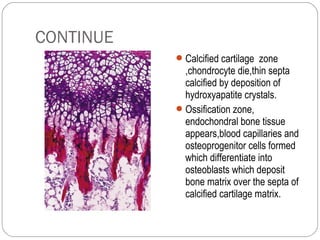





There are two main methods of ossification: intramembranous ossification and endochondral ossification. Intramembranous ossification forms flat bones directly from mesenchymal tissue through condensation, vascularization, osteoblast differentiation, and osteoid formation and calcification. Endochondral ossification forms long bones through a cartilage model, with primary ossification centers forming within the cartilage followed by invasion of blood vessels and osteoprogenitor cells leading to replacement of cartilage by bone except at joint surfaces. Growth in long bone length occurs through the epiphyseal plate where columns of chondrocytes undergo proliferation, hypertrophy, and calcification before being replaced by bone.























































































