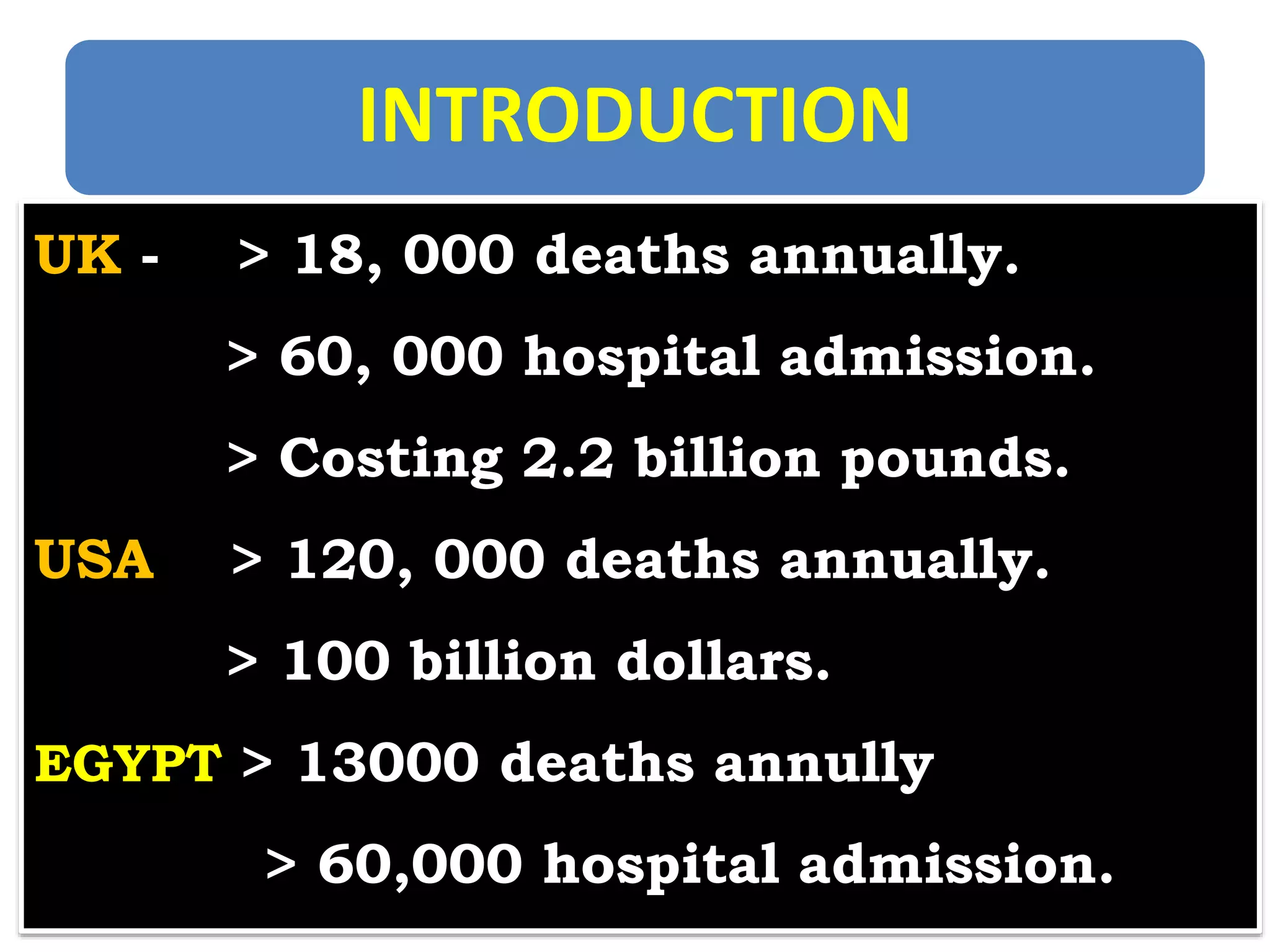
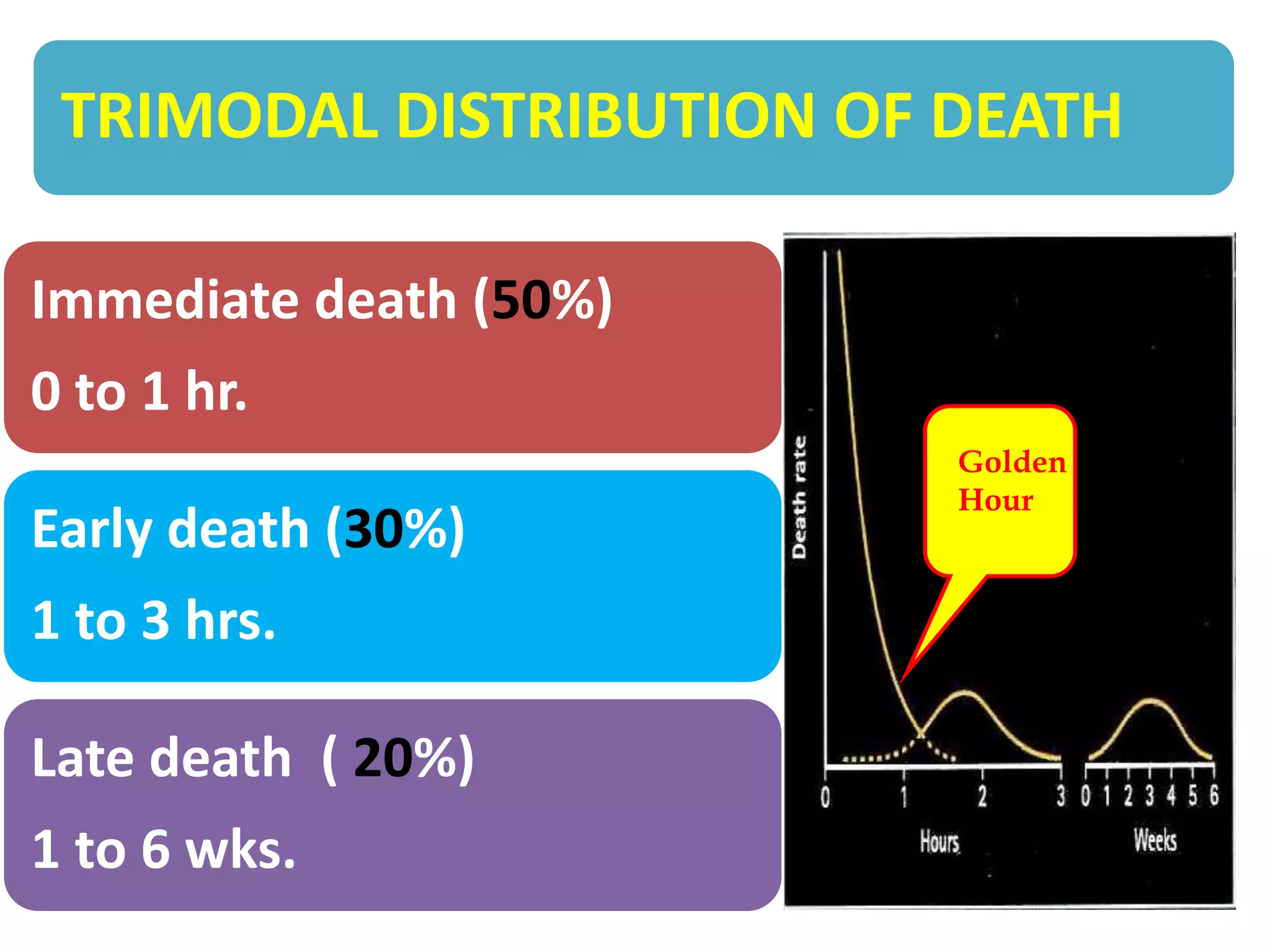
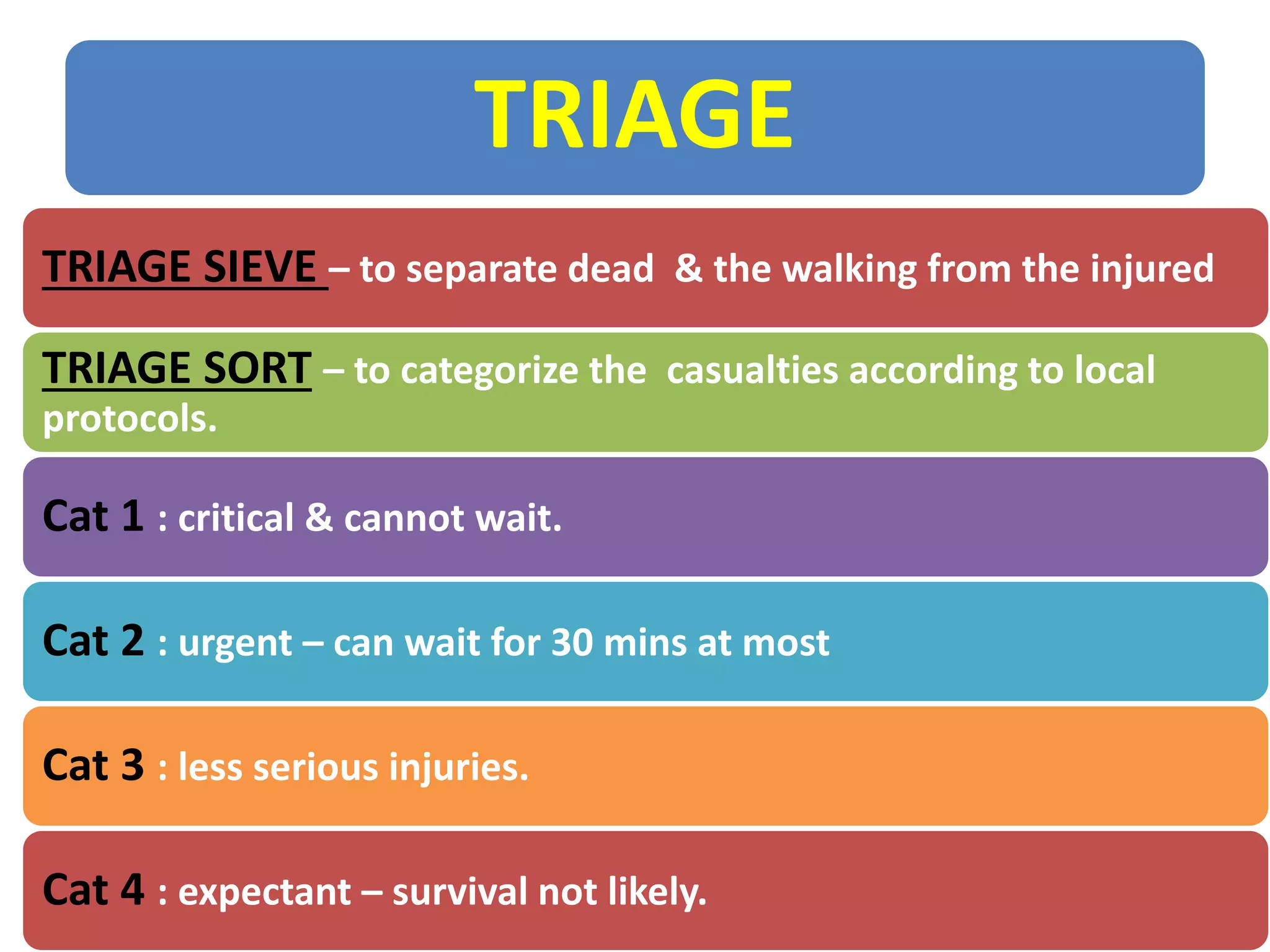
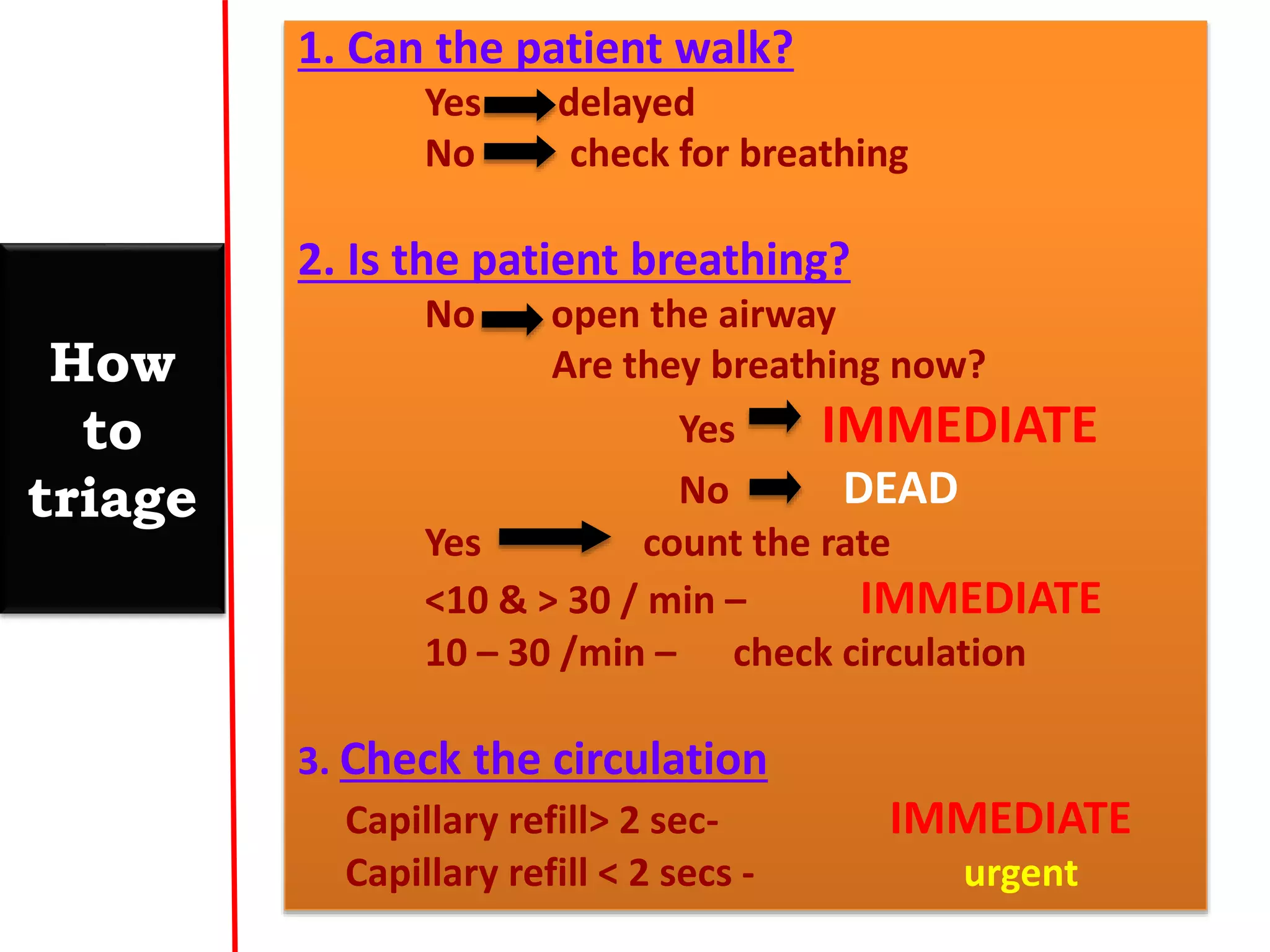
This document discusses trauma life support practices from Egypt to Ghana. It outlines the high rates of trauma deaths and costs in the UK and US, as well as trauma statistics in Egypt. It then covers mechanisms of injury, the trimodal distribution of death after trauma, and the steps of Advanced Trauma Life Support (ATLS). It also discusses prehospital retrieval and management approaches, levels of trauma centers, management in the hospital, the trauma team workflow and call-out criteria. It concludes with information on triage procedures and a proposed Facebook group for Egyptian and Ghanaian healthcare professionals.