Downloaded 30 times







![ Kussmaul breathing
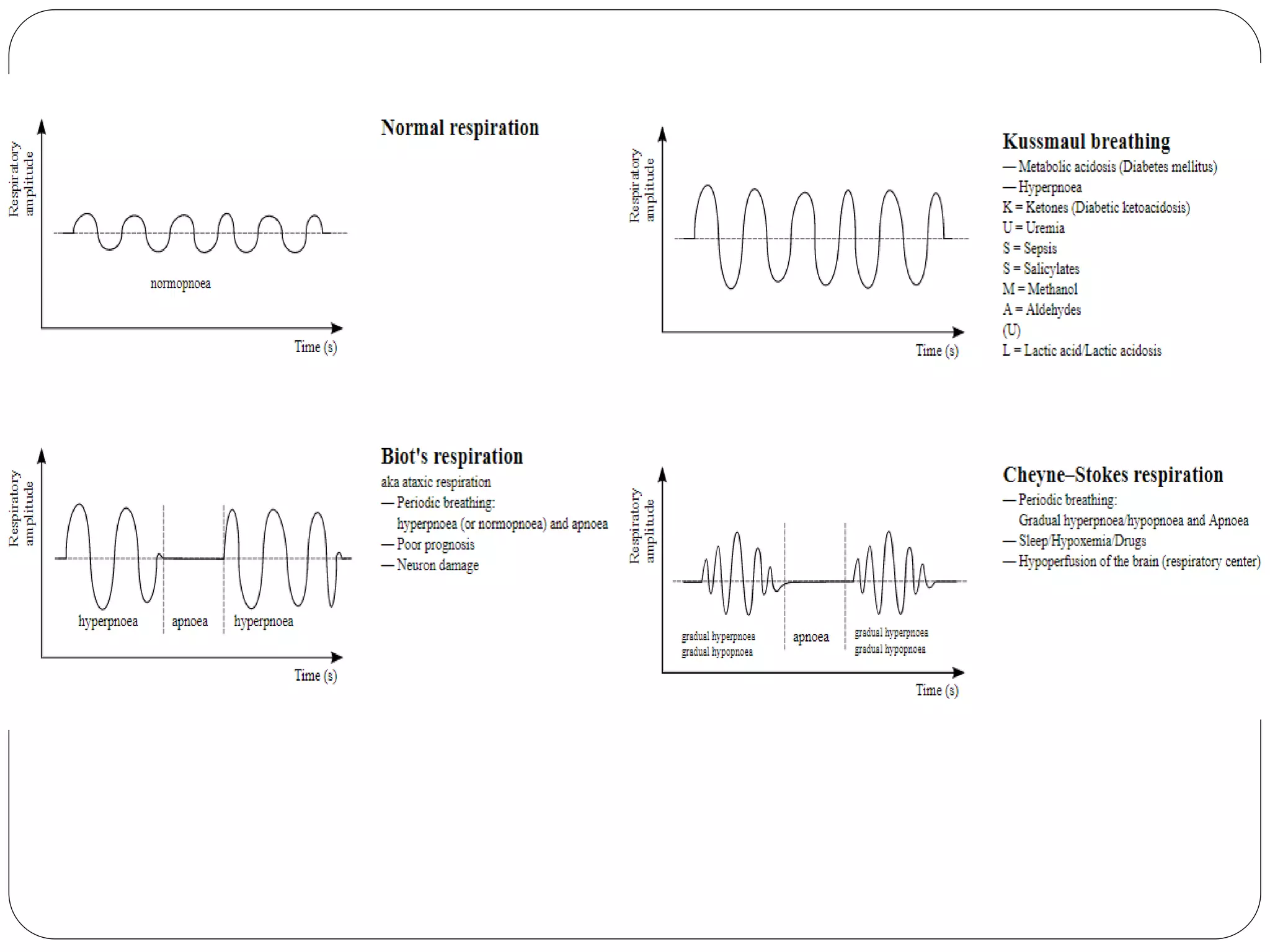
- It is a form of hyperventilation, which is any
breathing pattern that reduces carbon dioxide in
the blood due to increased rate or depth of
respiration.
- In metabolic acidosis, breathing is first rapid and
shallow[1] but as acidosis worsens, breathing
gradually becomes deep, labored and gasping.,
- Kussmaul breathing is respiratory compensation
for a metabolic acidosis, most commonly
occurring in diabetics in diabetic ketoacidosis .](https://image.slidesharecdn.com/respiratoryrate-201014170839/75/Respiratory-rate-16-2048.jpg)


The respiratory rate is controlled by the respiratory center located in the medulla oblongata and pons of the brain. The respiratory center receives input from chemoreceptors and mechanoreceptors to regulate breathing rate and depth. It is made up of groups of neurons that control inspiration and expiration. The normal respiratory rate varies by age but is typically 12-20 breaths per minute for adults. Deviations from the normal respiratory rate can indicate respiratory dysfunction and impact illness severity assessments.