Downloaded 478 times































































This document provides information on antimicrobial susceptibility testing using disk diffusion methods. It discusses the importance of AST for treating infectious diseases and monitoring antimicrobial resistance. The Kirby-Bauer disk diffusion method is described in detail, including media preparation, inoculum standardization, disk and antibiotic solution preparation, quality control strains, incubation, reading zones of inhibition, and interpreting results according to CLSI guidelines. Special considerations are given to organisms like MRSA, VISA, and inducible clindamycin resistance in Staphylococci.
Introduction to antimicrobial susceptibility testing (AST) methods, importance in treatment and resistance monitoring.
AST guides antibiotic selection, gathers epidemiological data on microbial resistance for public health.
Defining AST: measuring minimum inhibitory concentration. Importance of quality control in laboratory testing.
Various AST methods including disk diffusion (Kirby-Bauer, Stokes), MIC, and E-test.
Explanation of Kirby-Bauer disk diffusion method principle, antibiotic diffusion, and organism susceptibility.
Muller Hinton Agar specifications for non-fastidious organisms, its reproducibility, and quality check details.
Guidelines for receiving, storing, and preparing antibiotic disks including homemade disks.
Standards for preparing inoculum turbidity using McFarland Standards, essential for accurate AST.
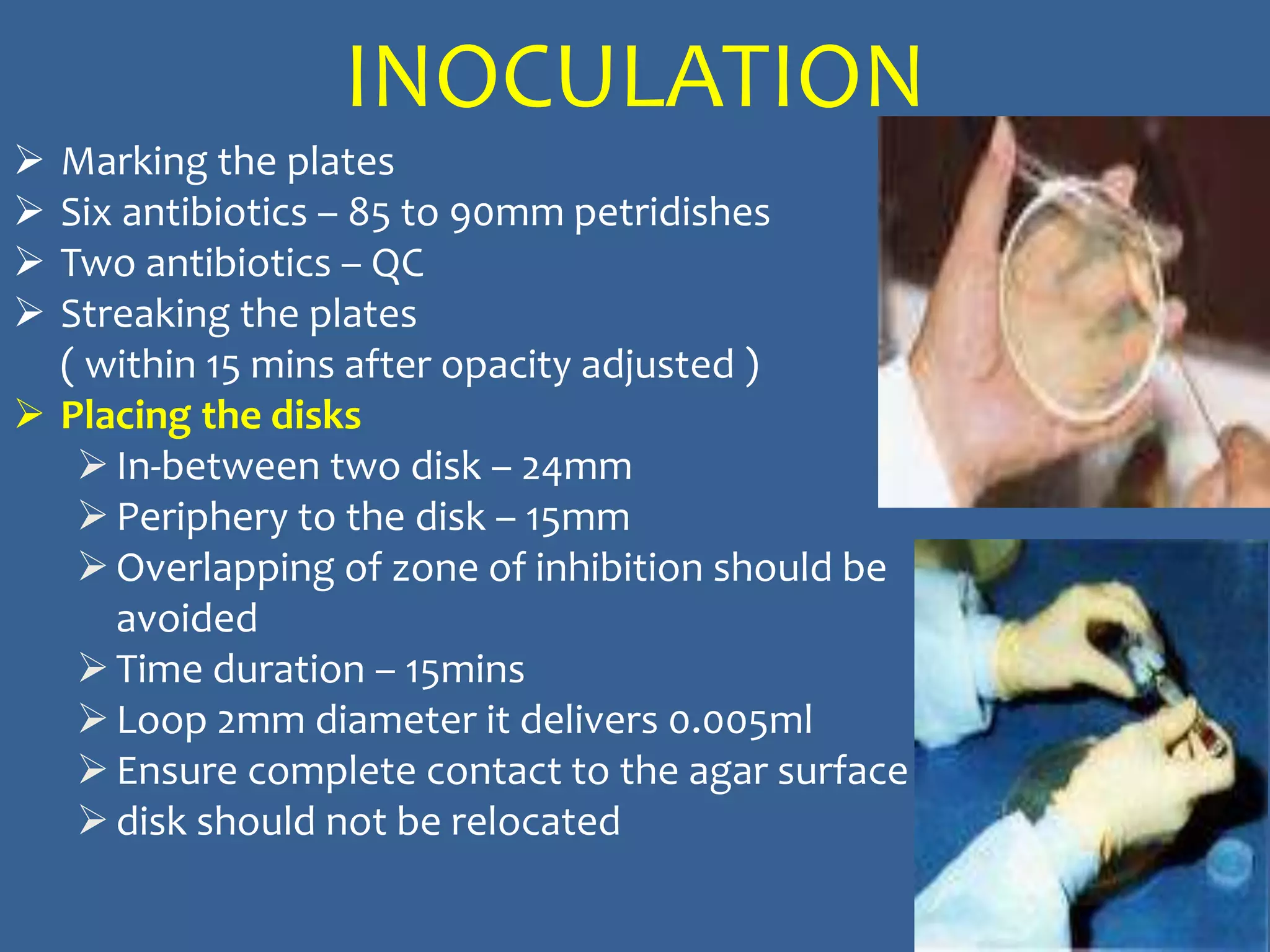
Techniques for inoculating plates with bacteria, placement of disks, and incubation guidelines.
Importance of quality control in AST, assessment of standard strains, and ensuring reliable results.
Guide to reading AST results based on zone sizes and organism response based on CLSI guidelines.
Influences on inhibition zones including cations, medium depth, and inoculum preparation errors.
Review of potential results interpretation errors, resistant mechanisms, and implications for treatment.
Methods for MRSA detection, mechanisms of resistance including mecA gene and implications for treatment.
Detection and implications of vancomycin resistance in S.aureus strains and detection methods.
Mechanism of ESBL production, impact on treatment, and testing methods to detect resistant strains.
High-level aminoglycoside resistance in enterococci, detection methods, and treatment guidelines.















































![Antibiotic assay, sensitivity and chemotherapy [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/antibioticassaysensitivityandchemotherapyautosaved-210119212020-thumbnail.jpg?width=640&height=640&fit=bounds)



















