






























































































The document discusses various techniques for limb salvage surgery following bone tumors. It describes the principles of limb salvage compared to amputation, including survival, recurrence, function, and complications. Various reconstruction options after tumor resection are summarized, including allografts, vascularized bone grafts, prosthetics, arthrodesis, rotationplasty, and total femur replacement. Specific case examples illustrate different reconstruction techniques for various tumor locations.
Overview of limb salvage approach and its significance in orthopaedic practices.
In the 1970s, amputation was the standard treatment for limb conditions.
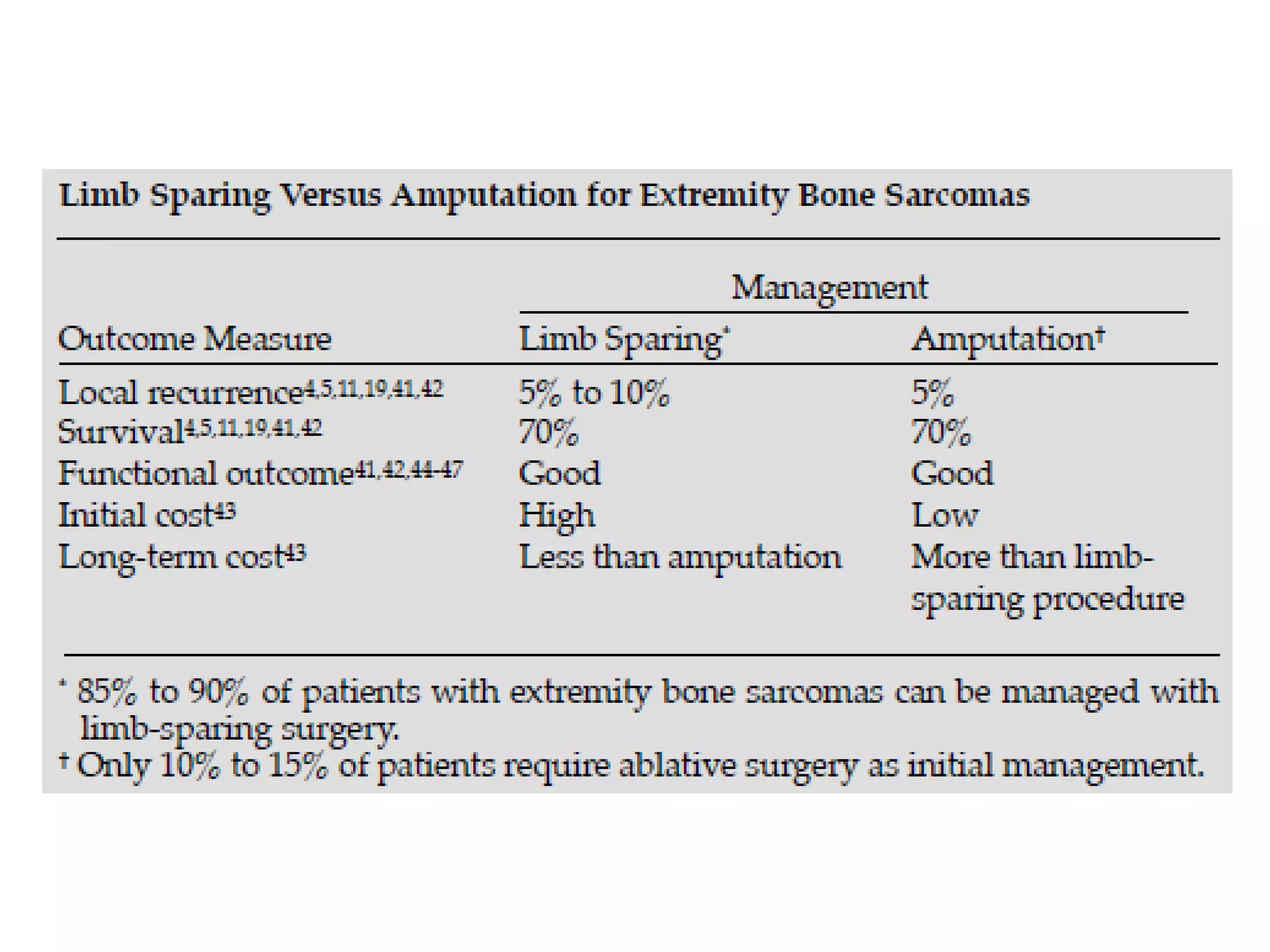
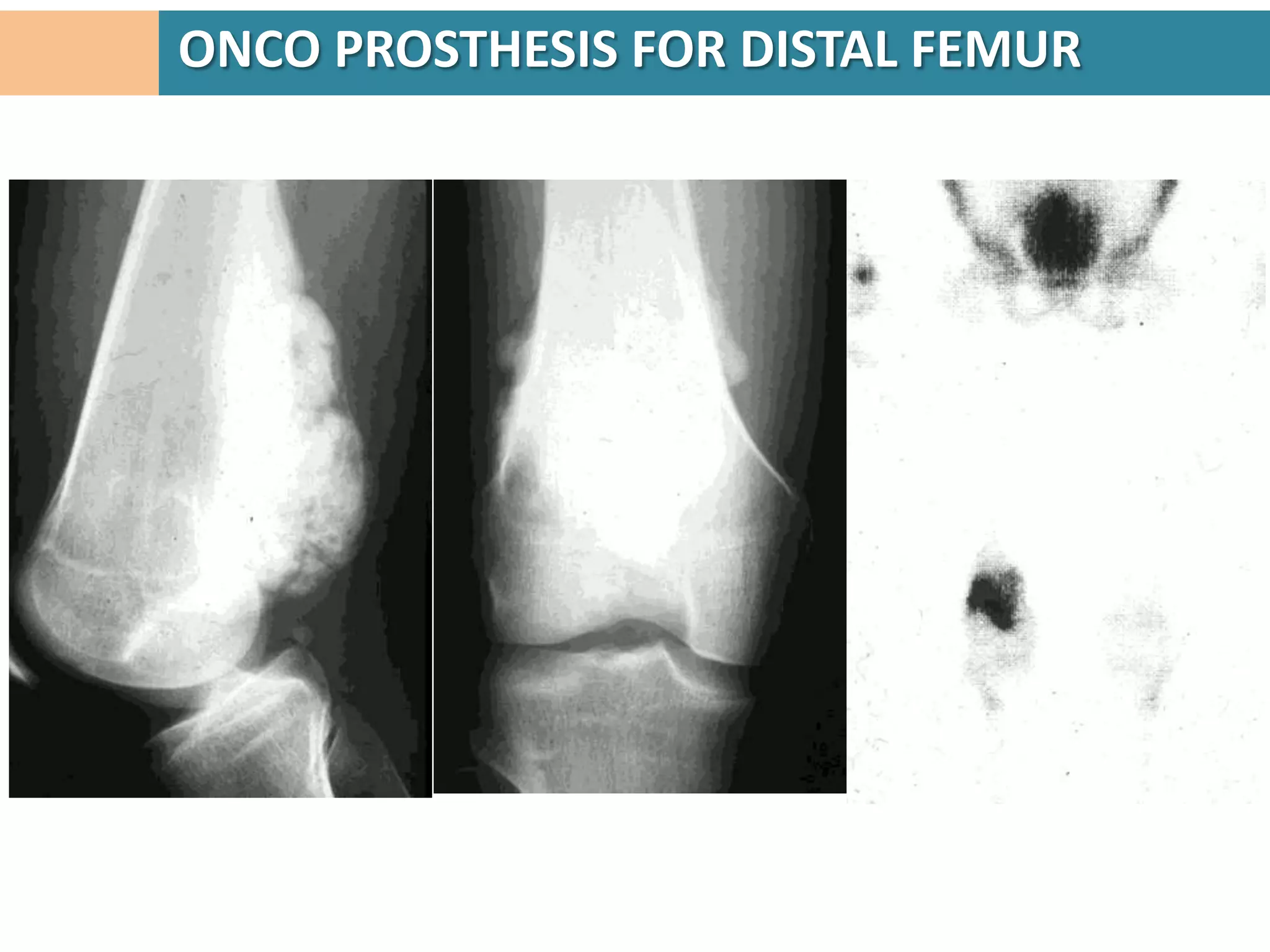
Key principles include comparisons with amputation, contraindications, and surgical evaluations.
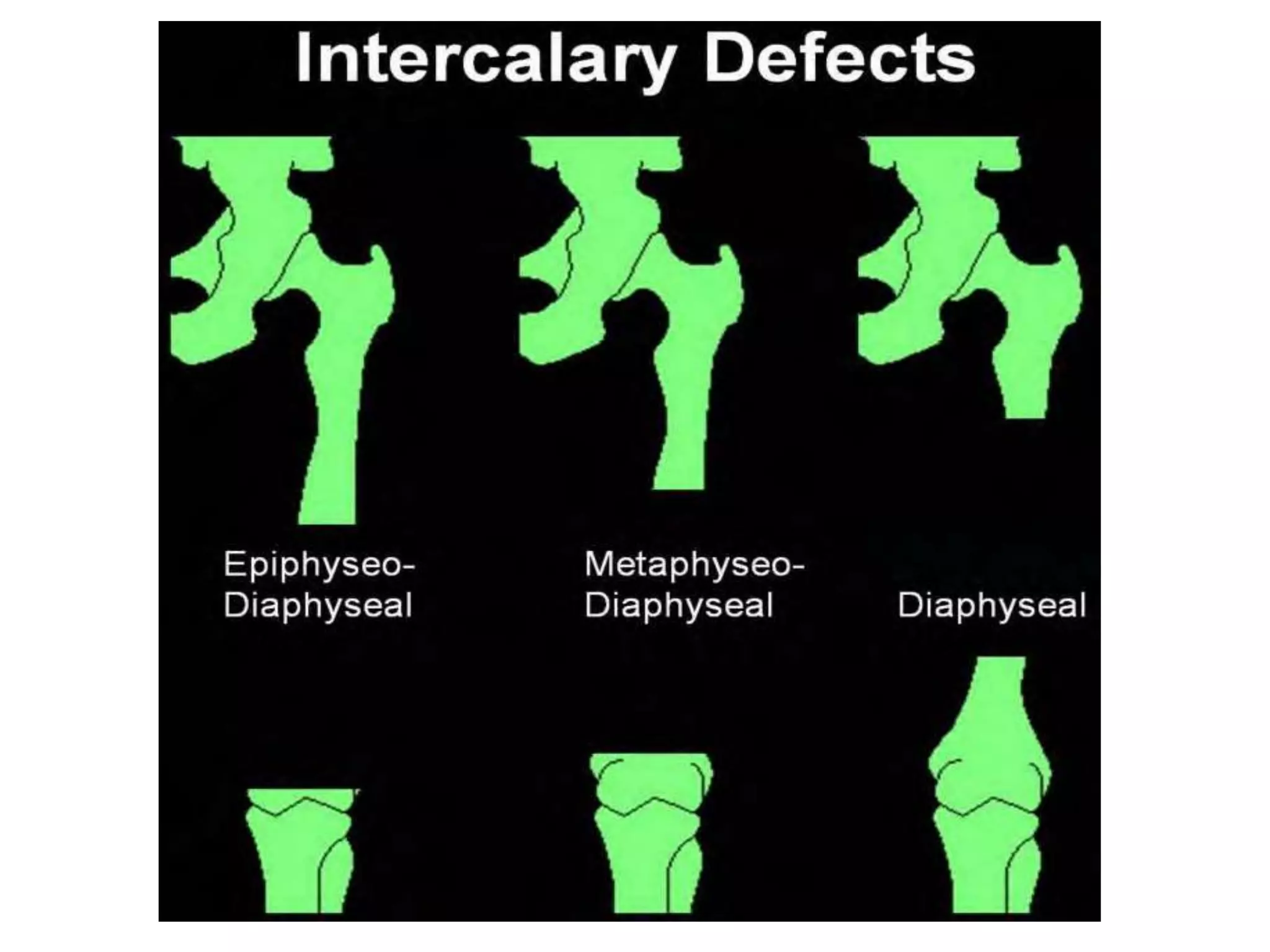
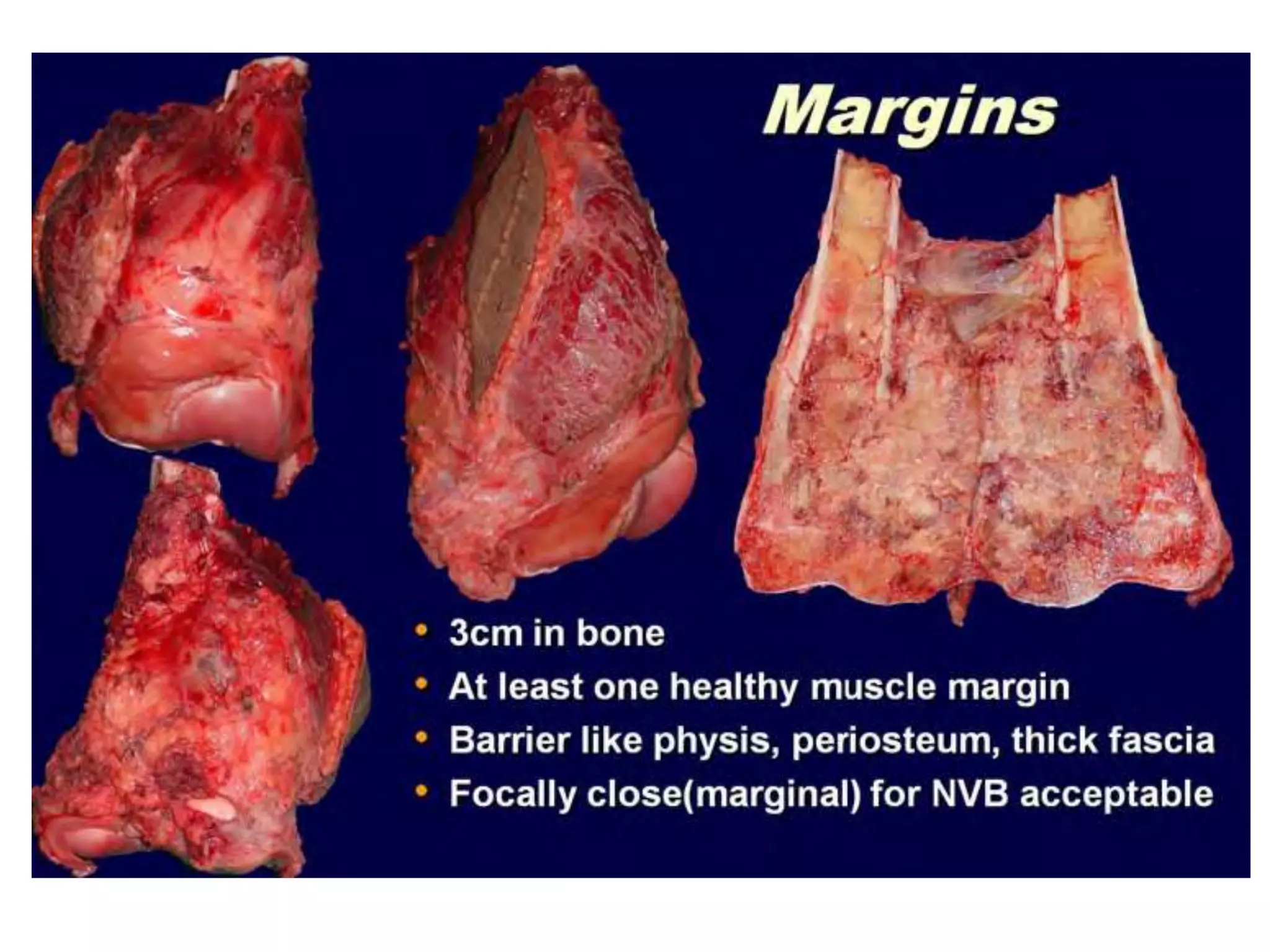
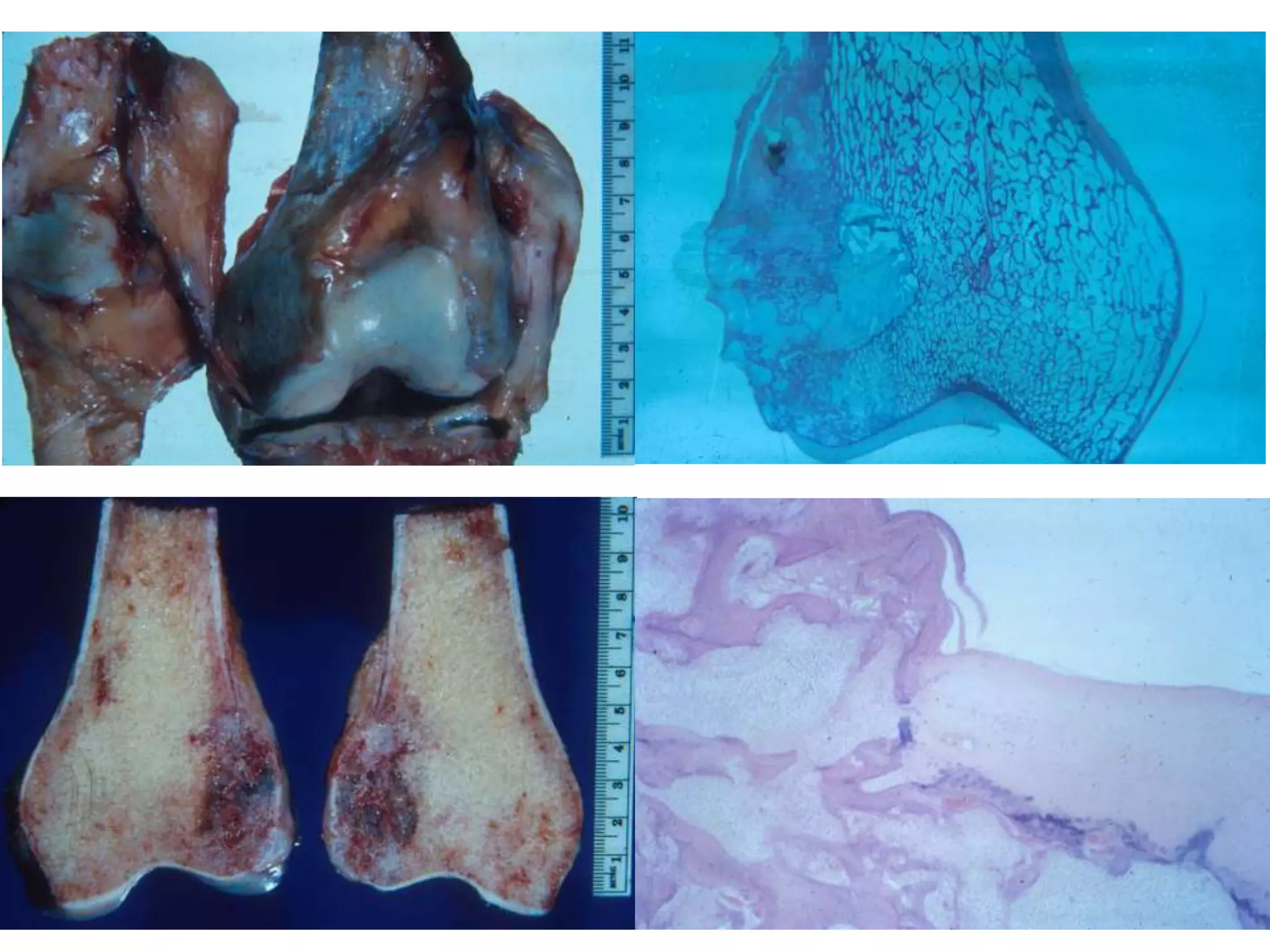
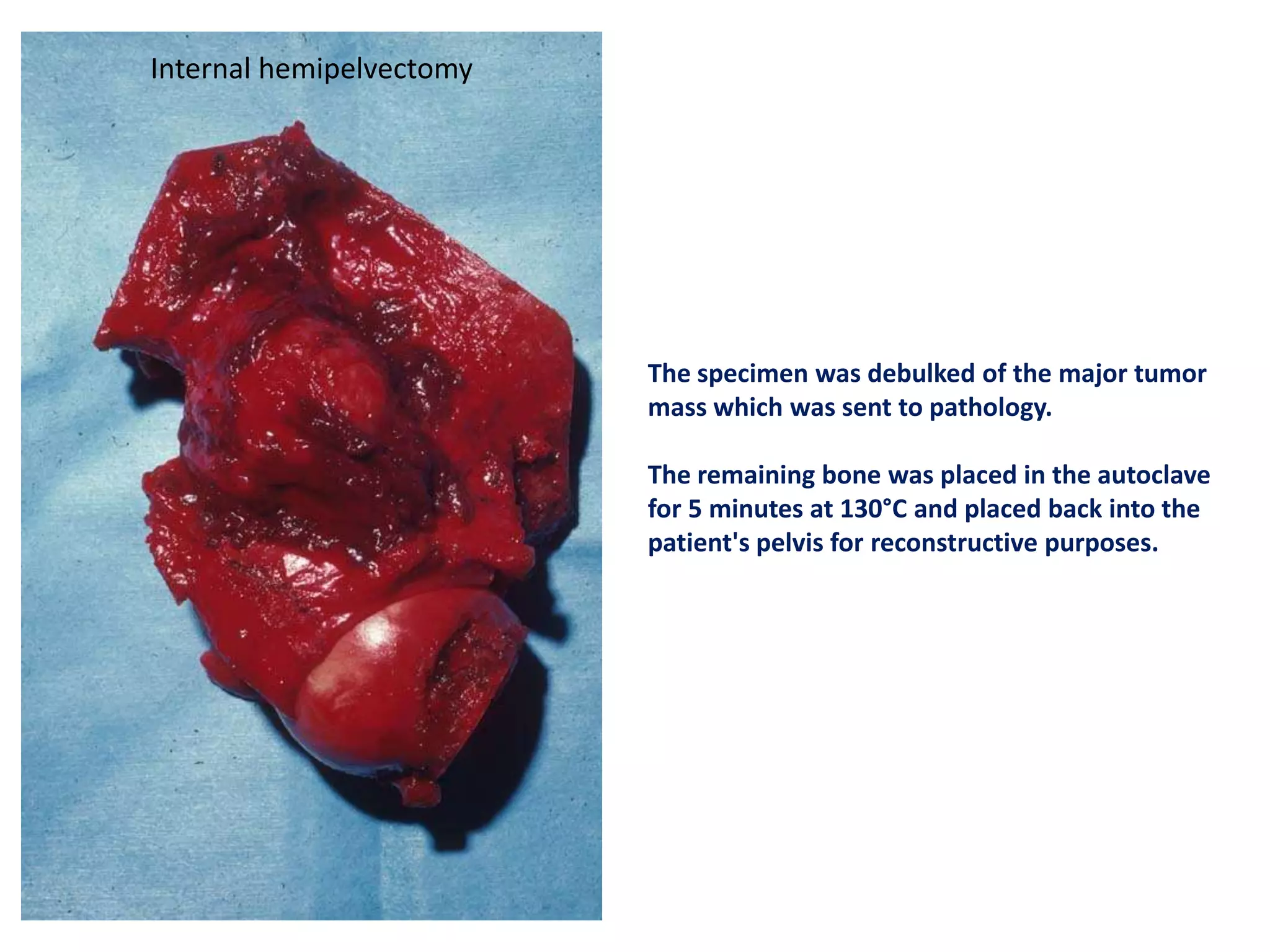
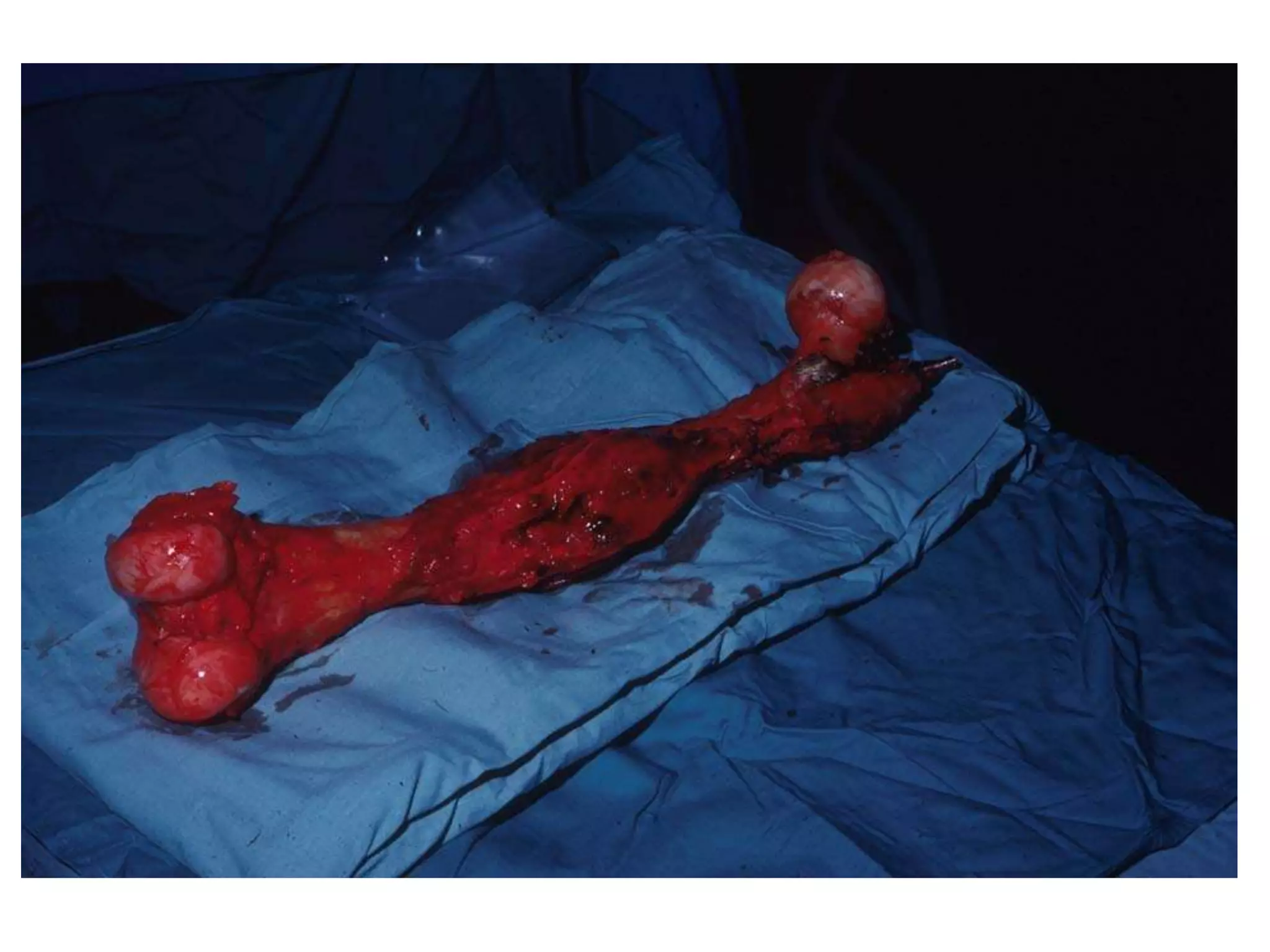
Discusses resection, fixation methods like external fixators, and use of autografts.
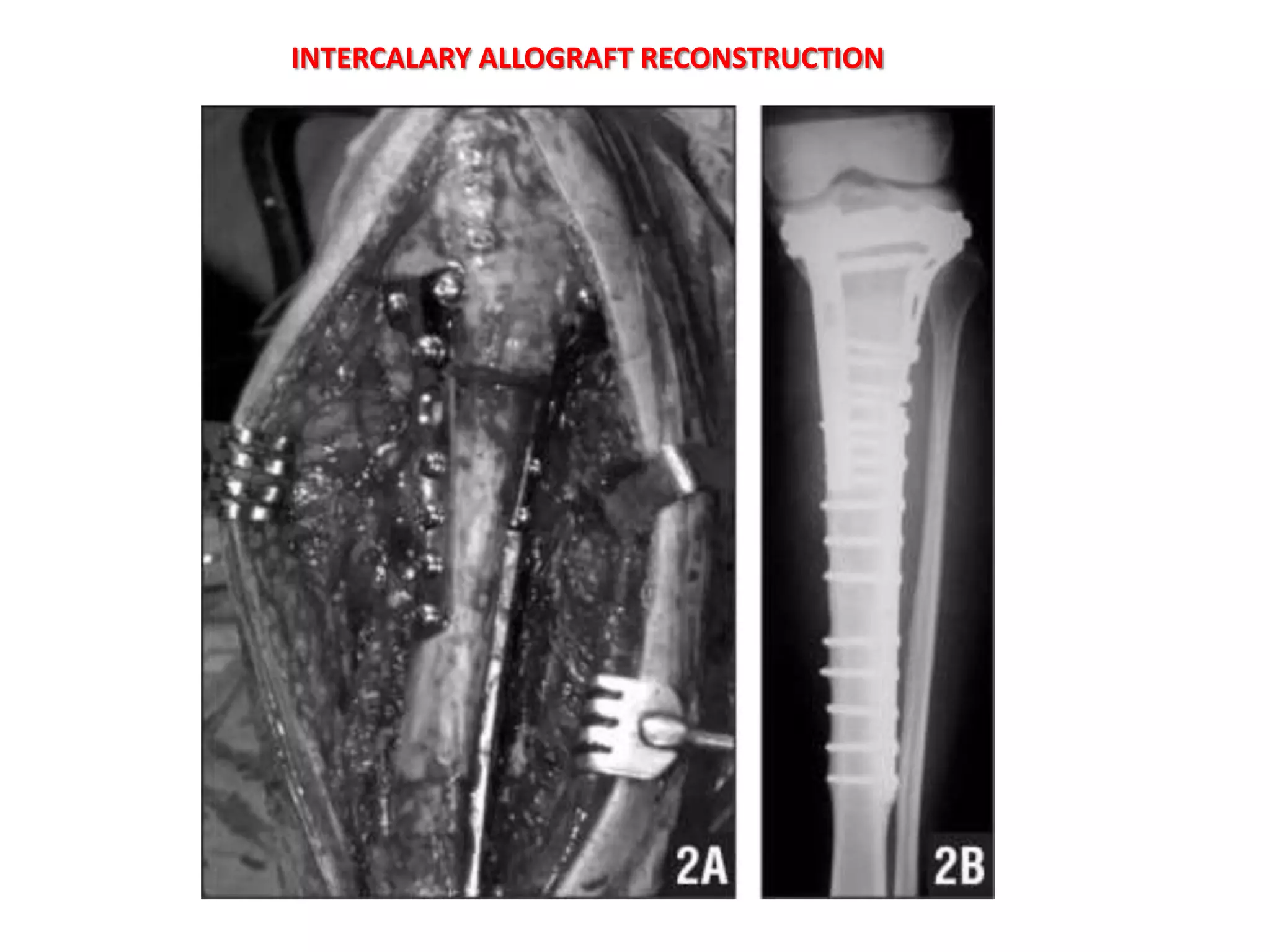
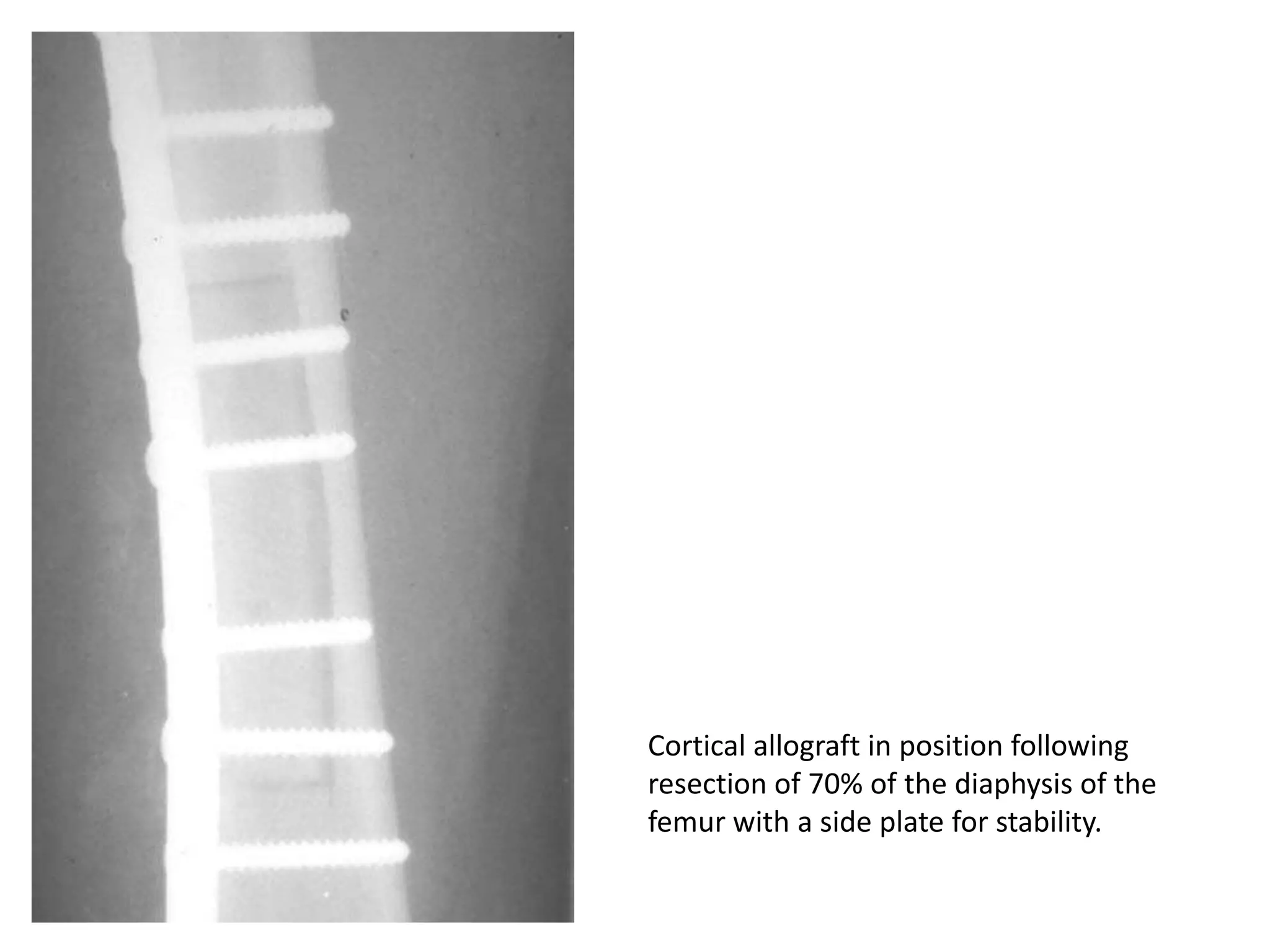
Various reconstruction methods like autografts, bone cement, and allografts are explored.Challenges in allografting such as infection risks and incorporation issues.
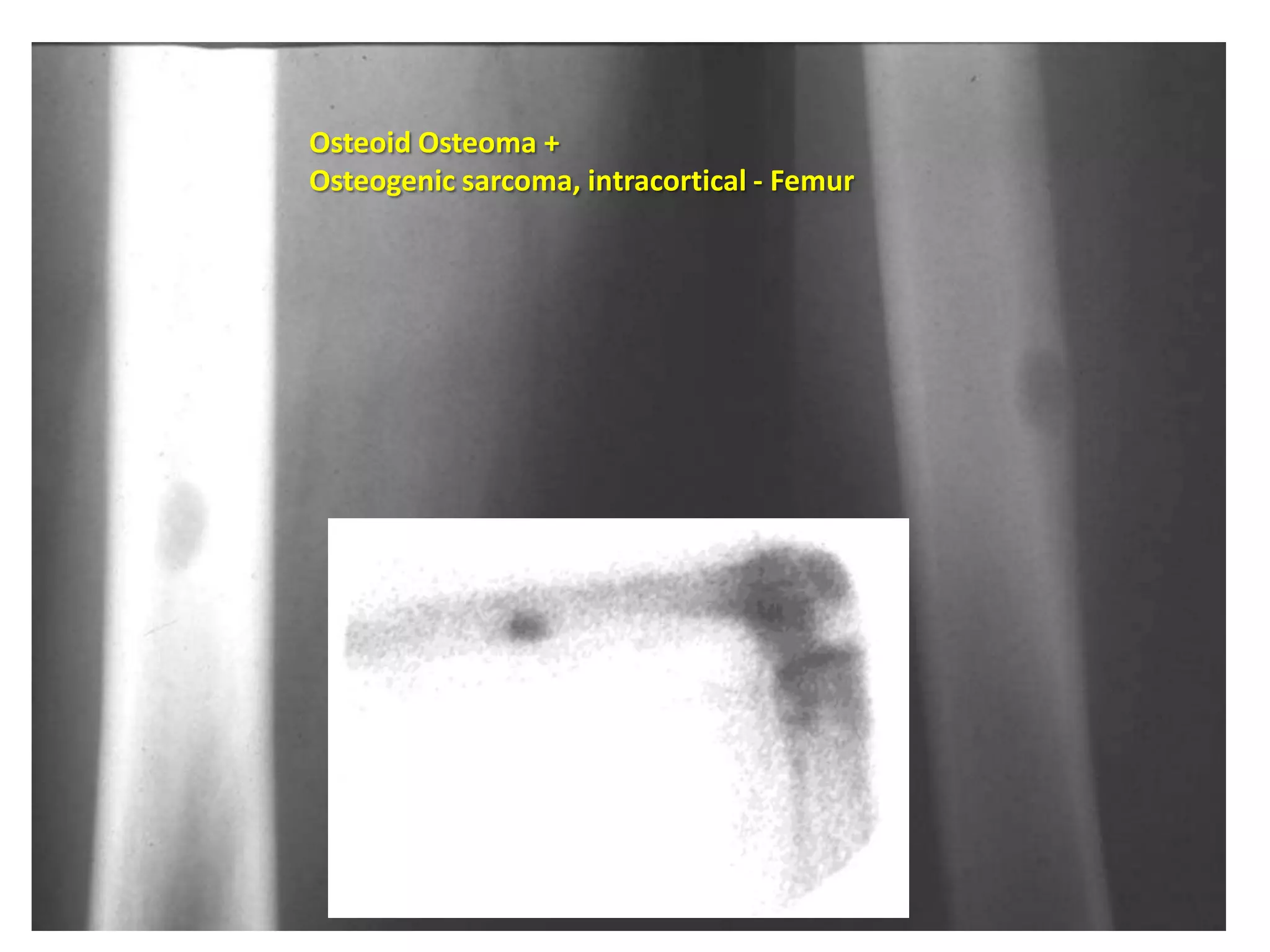
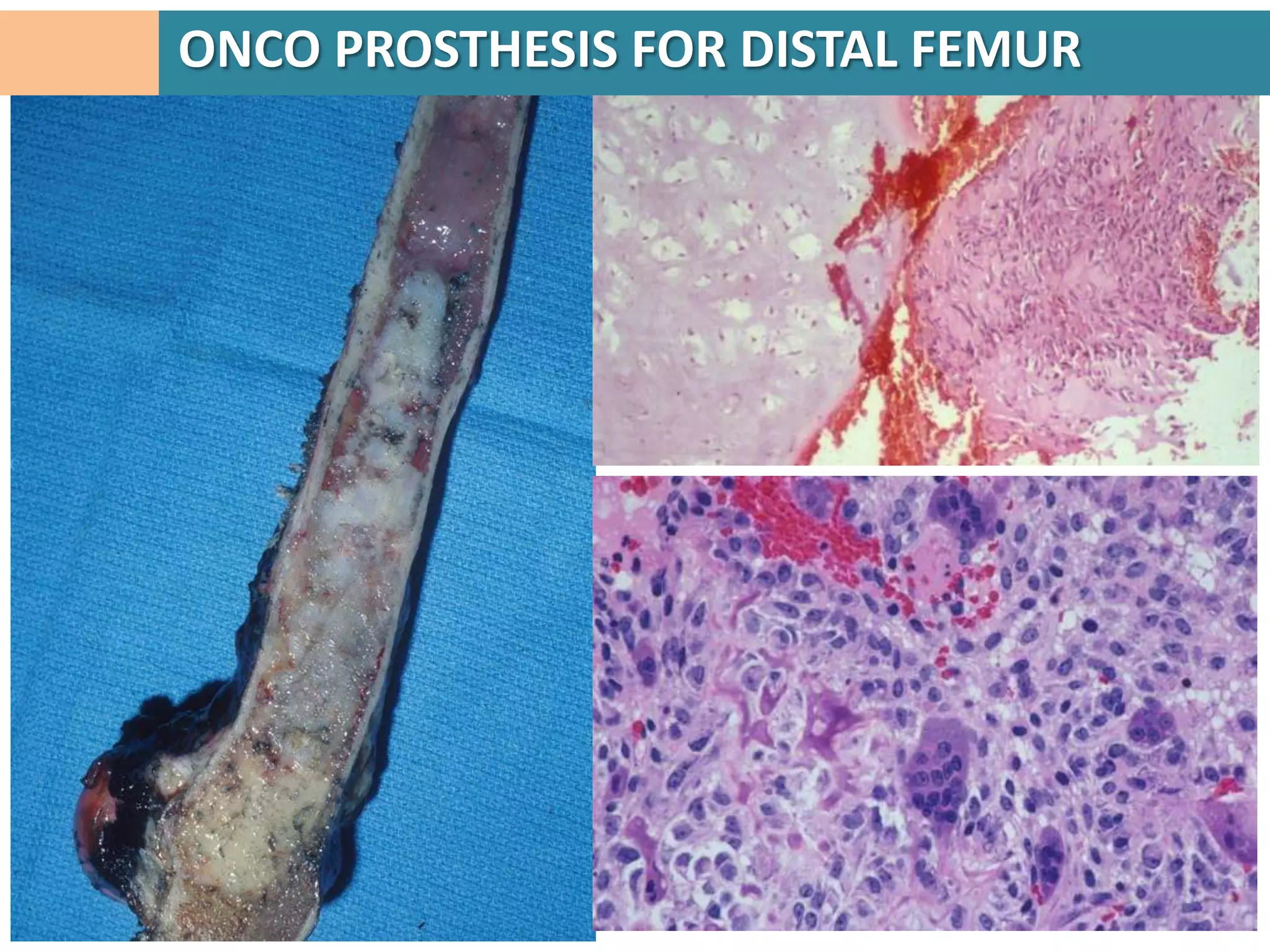
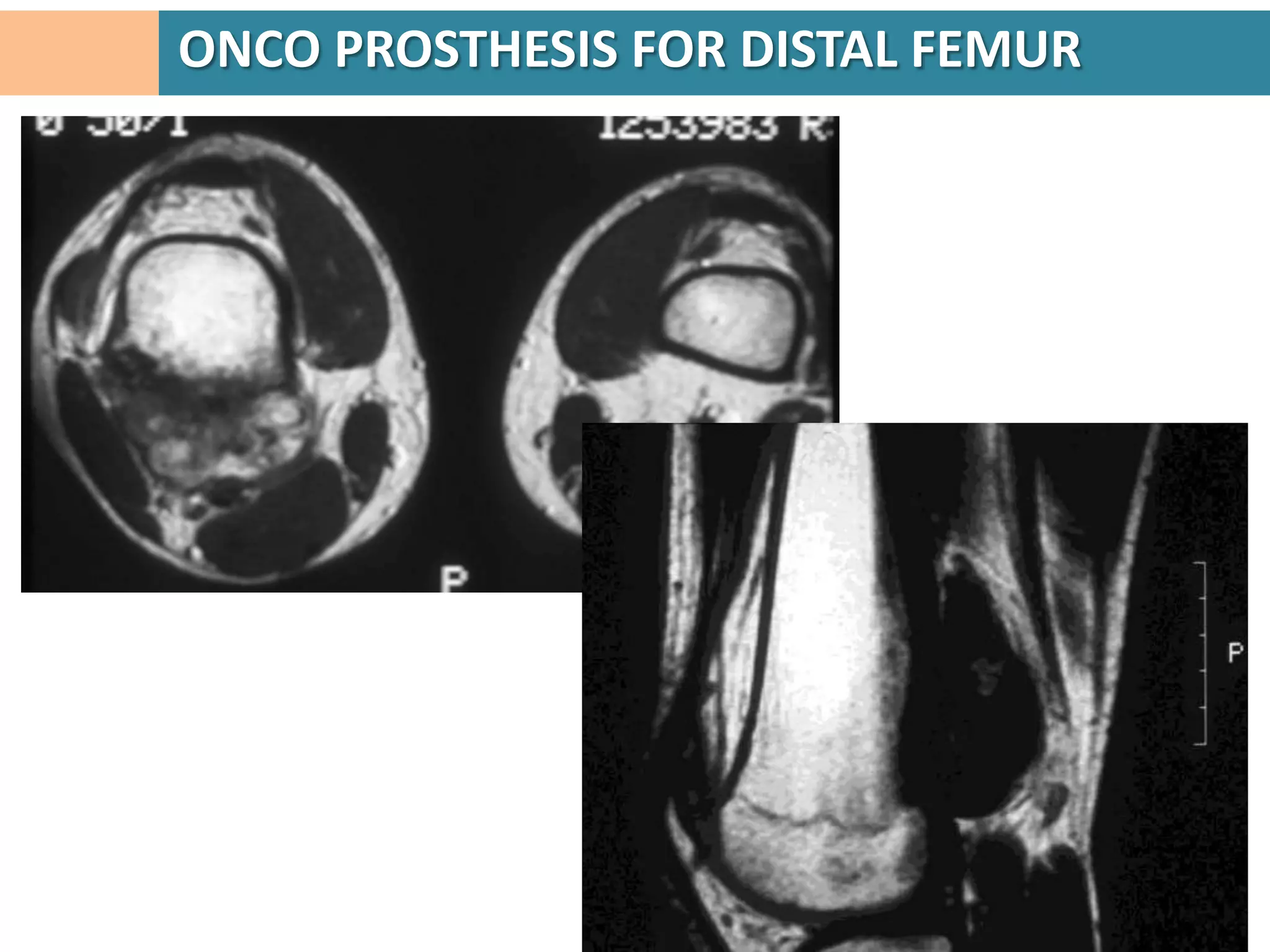
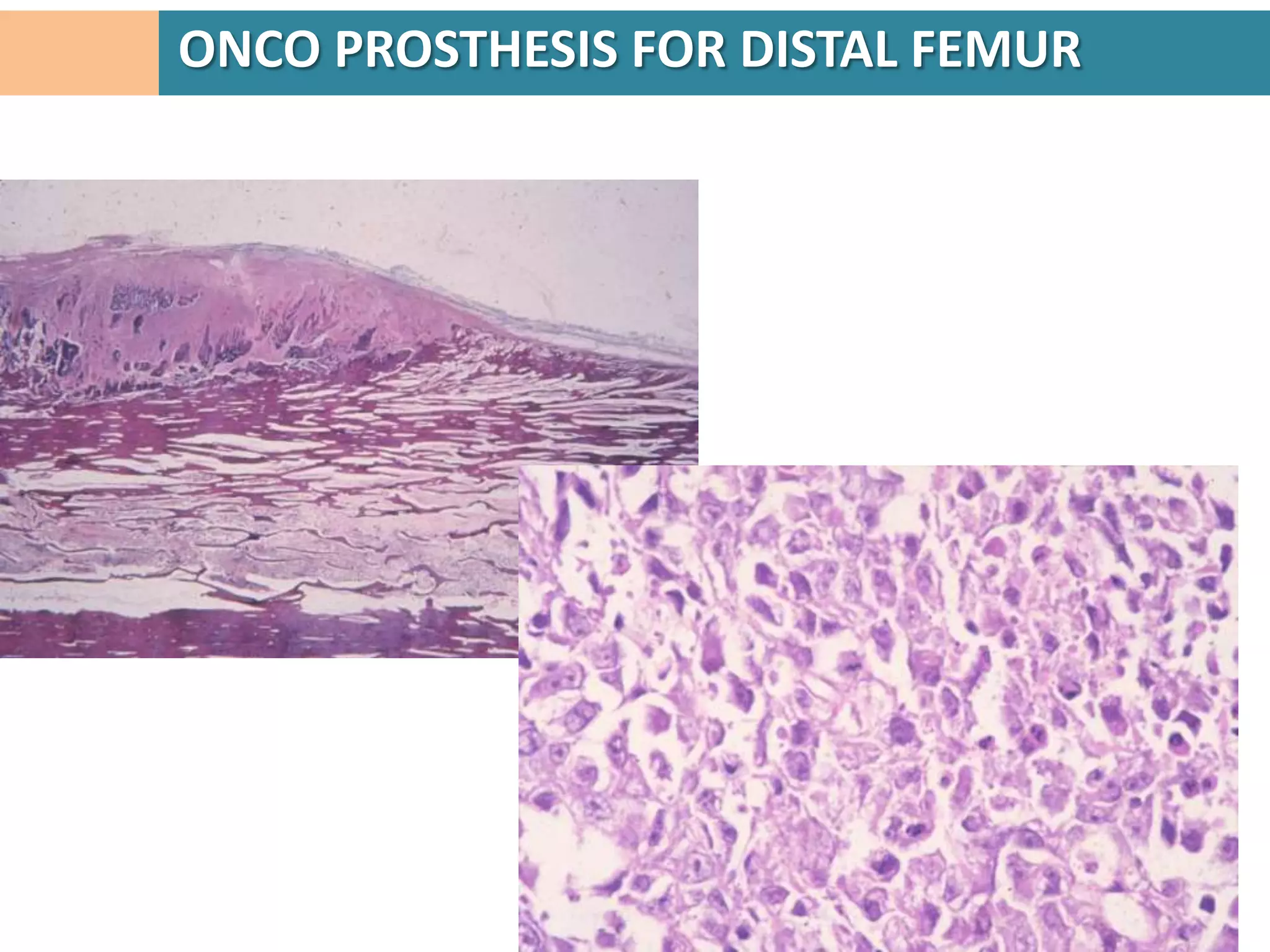
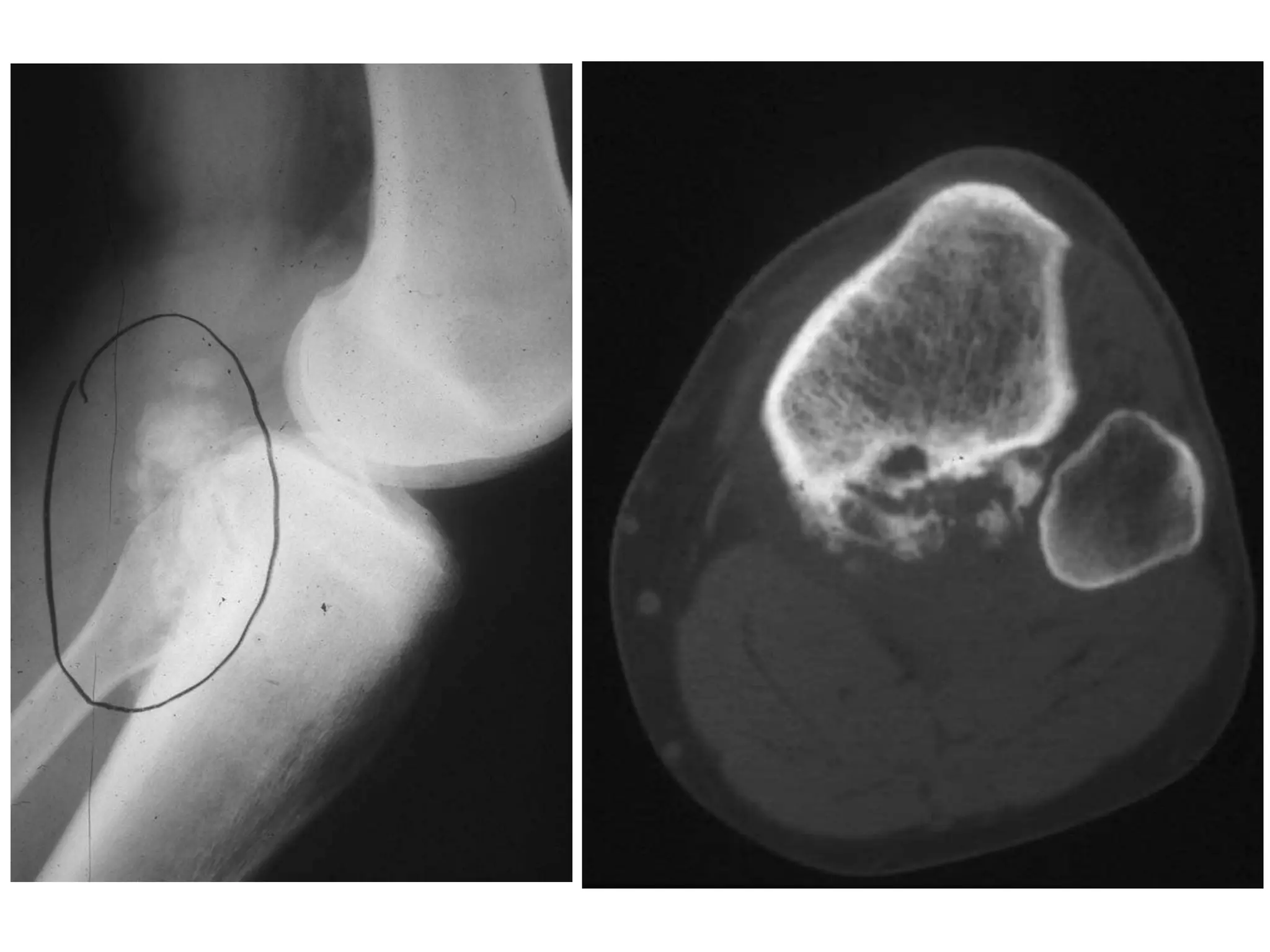
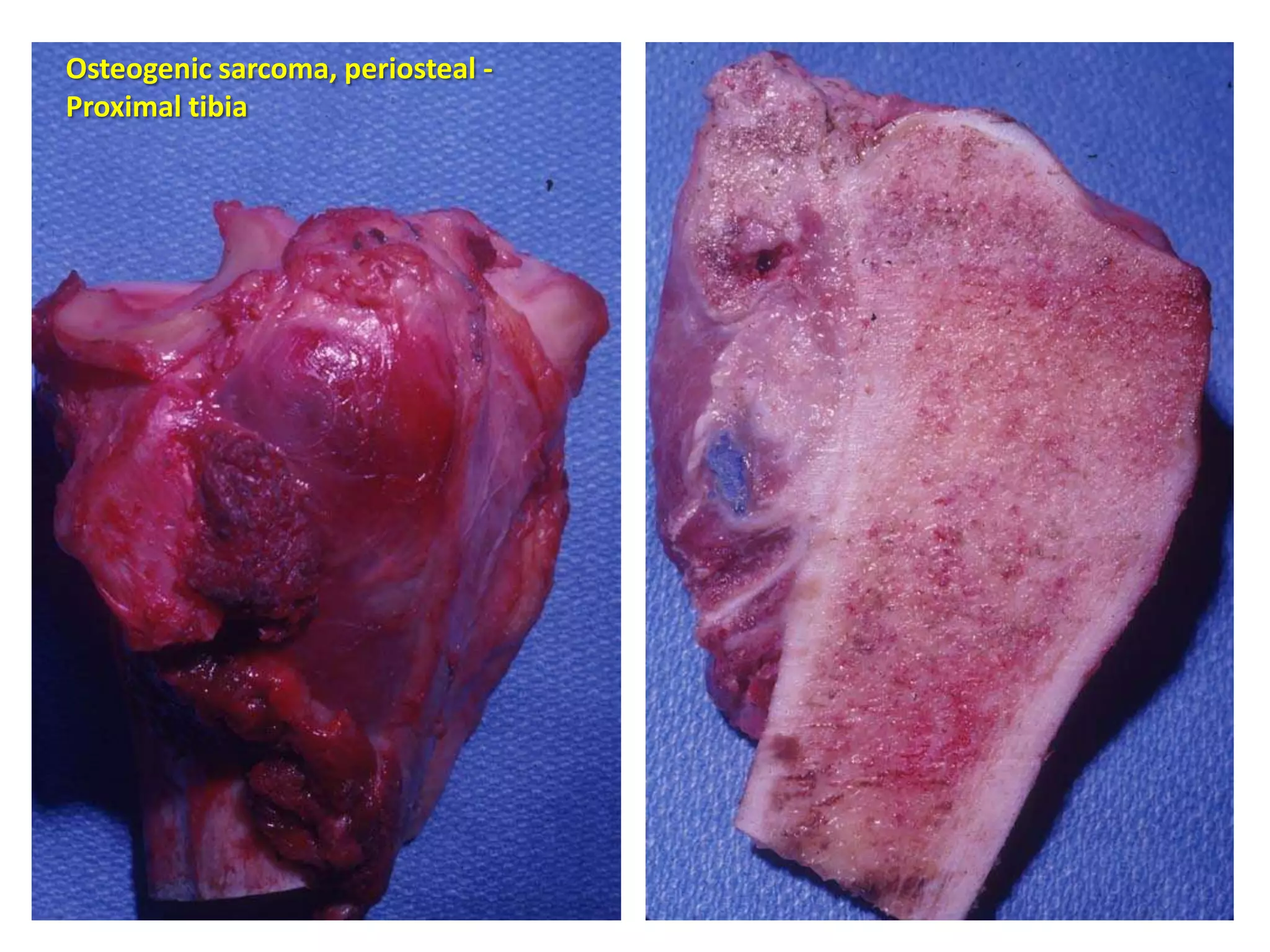
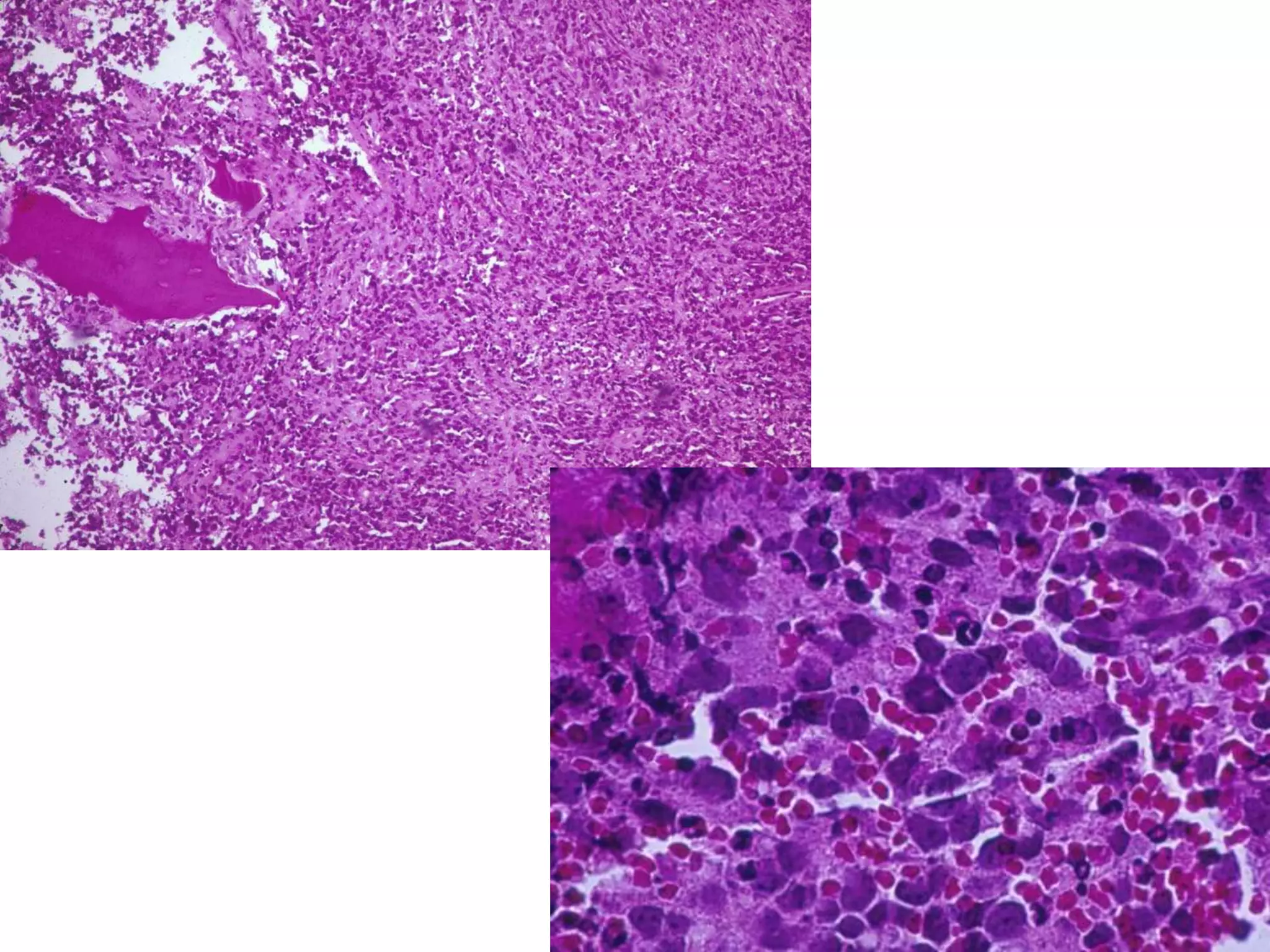
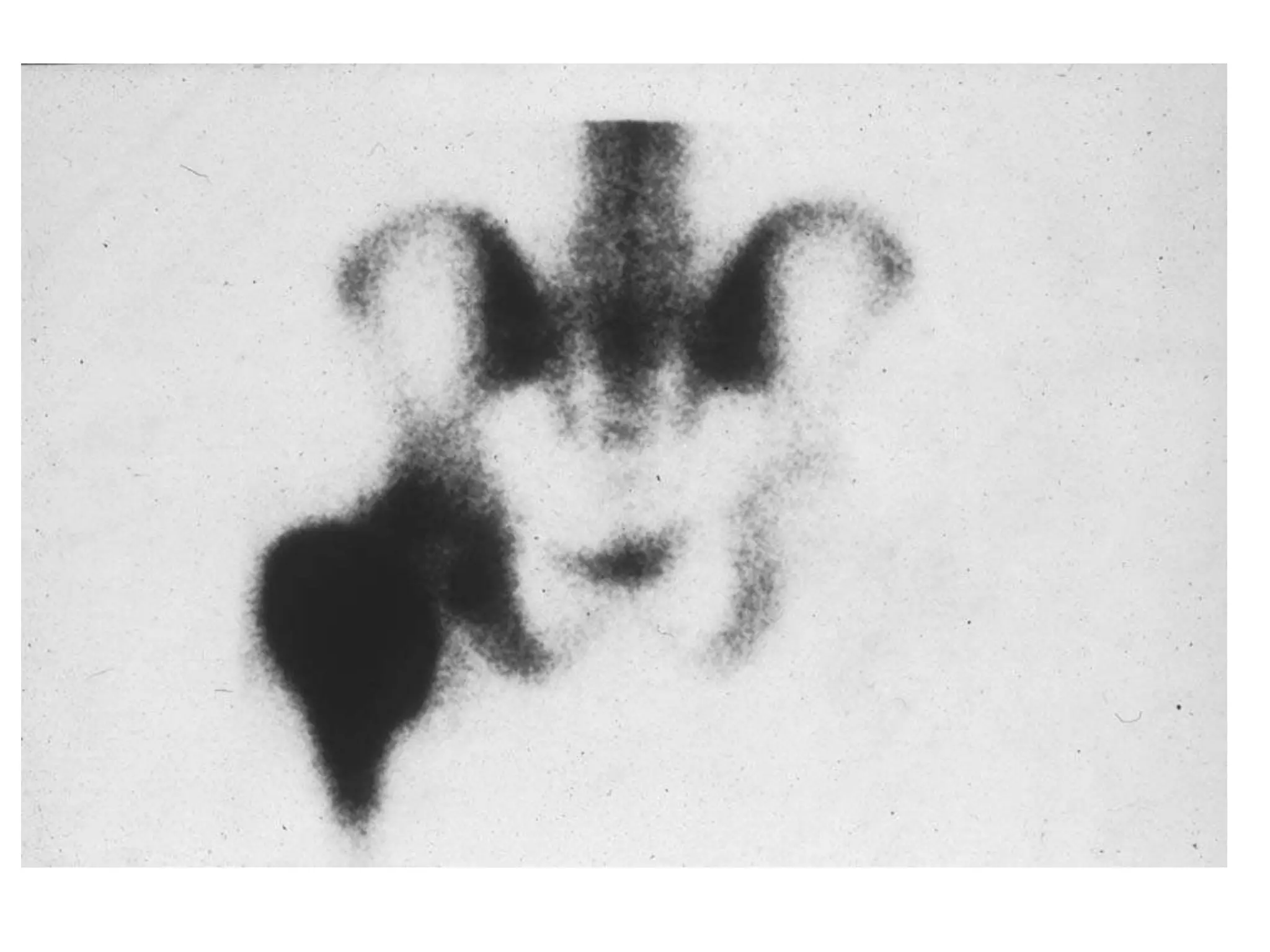
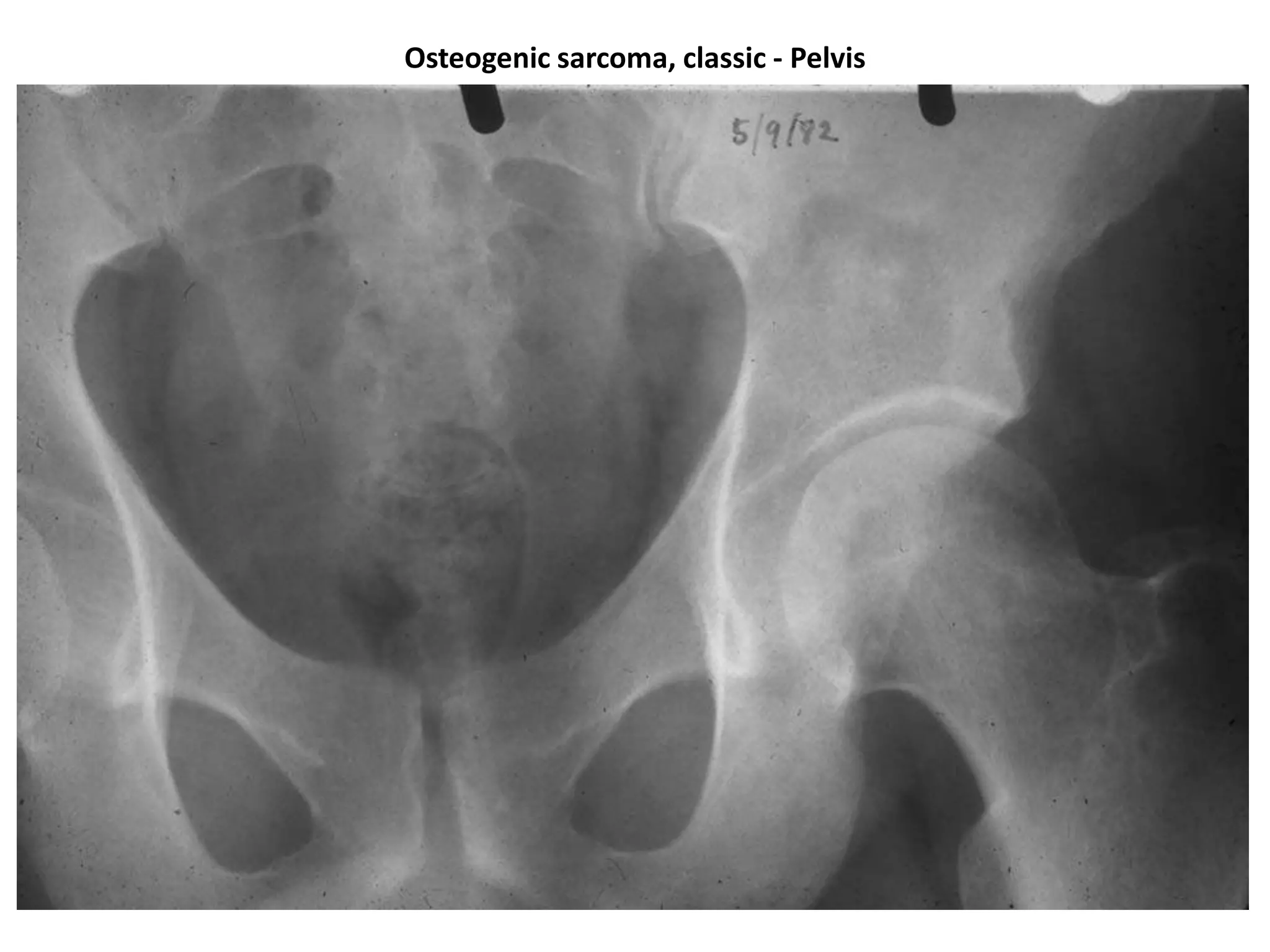
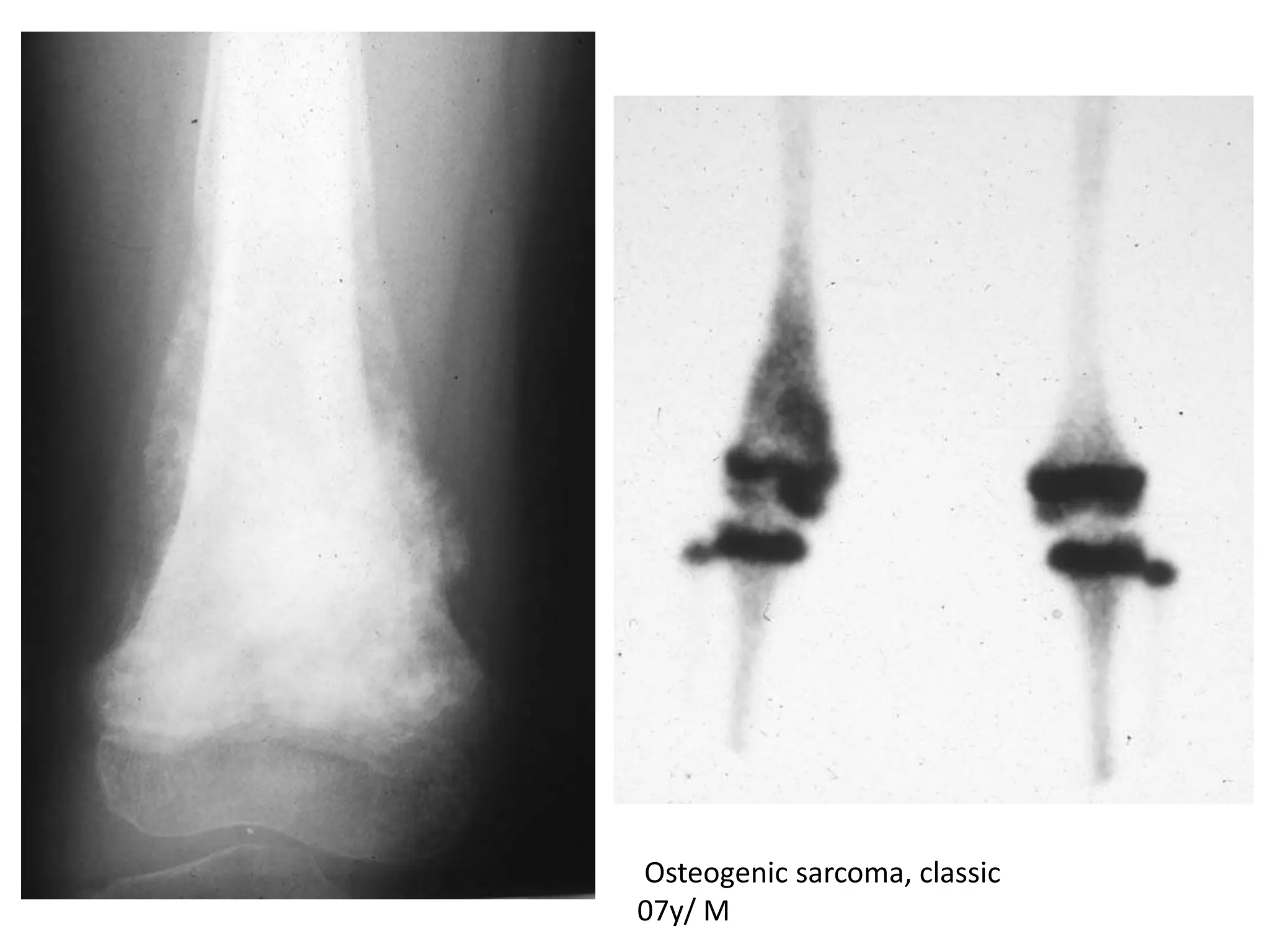
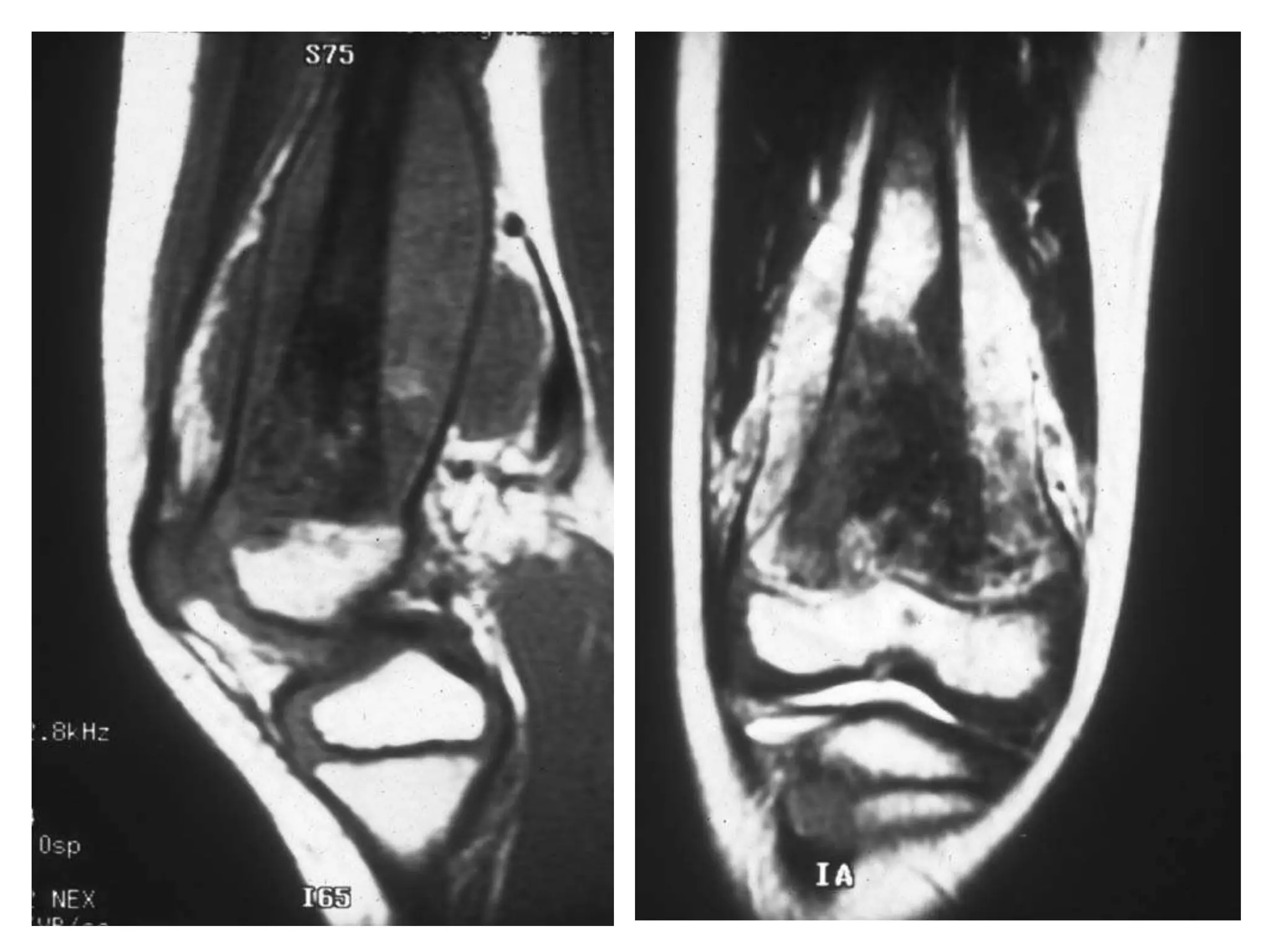
Discussion on reconstructive approaches following tumor resections in cases like osteoid osteoma.
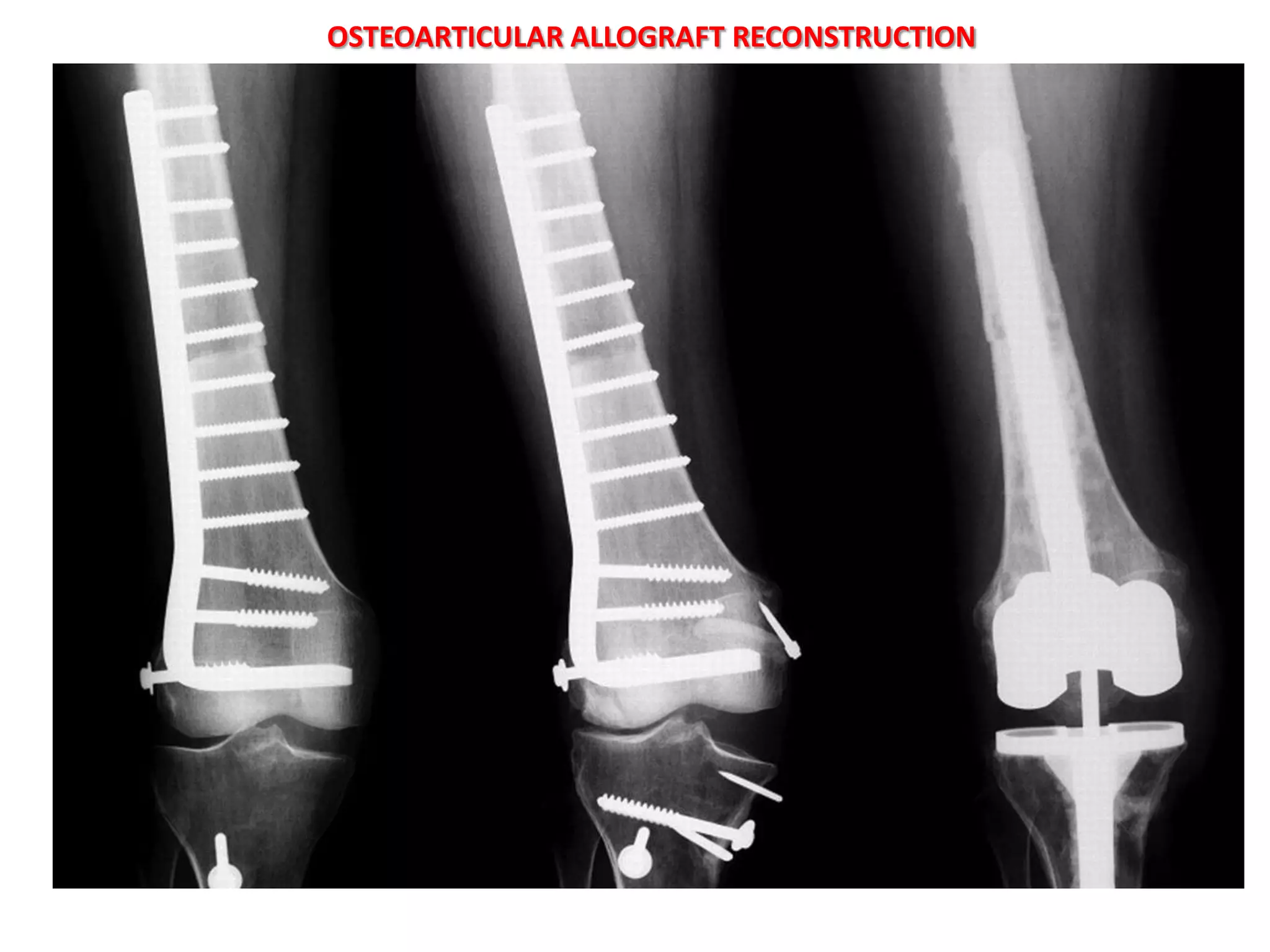
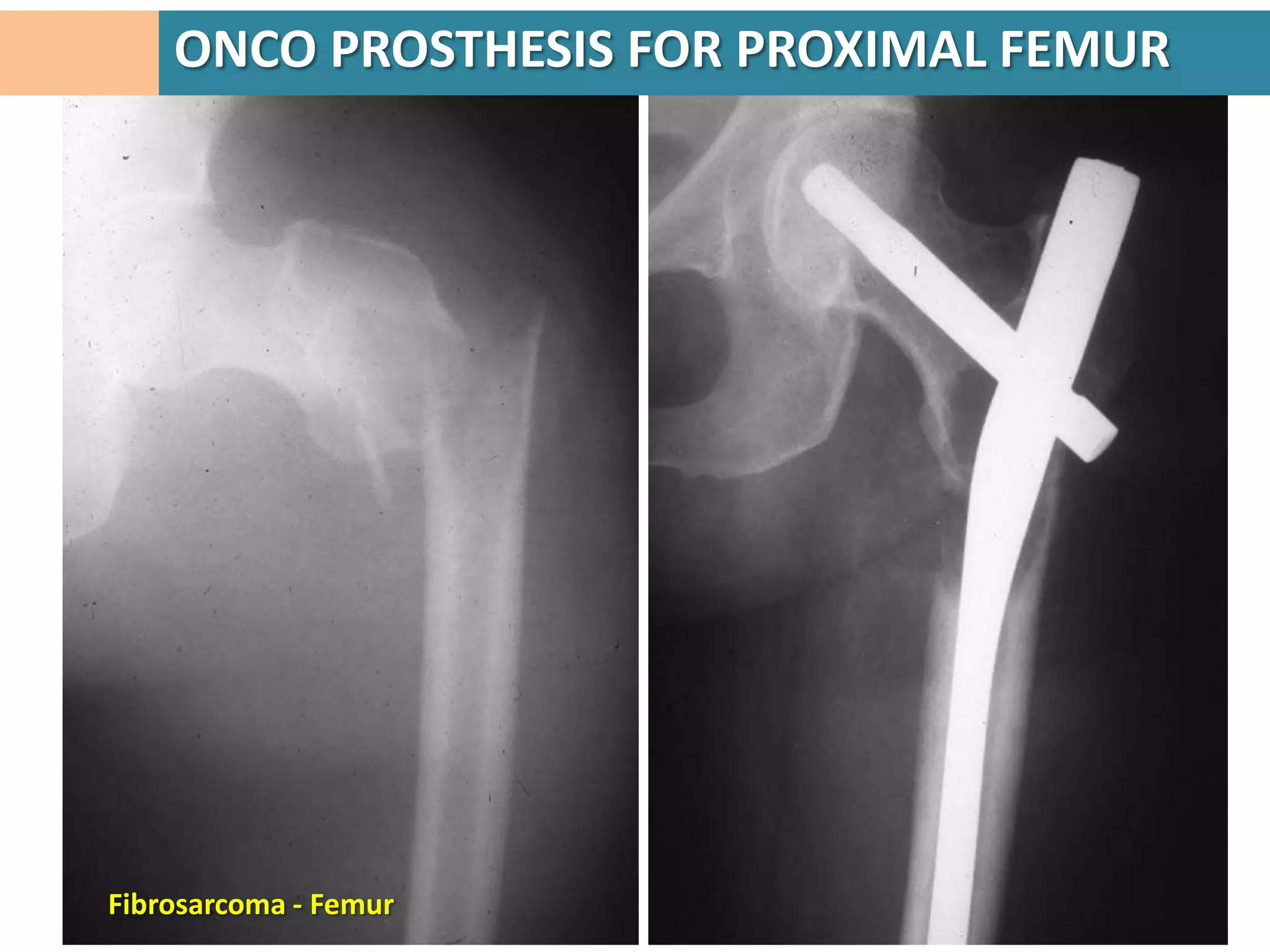
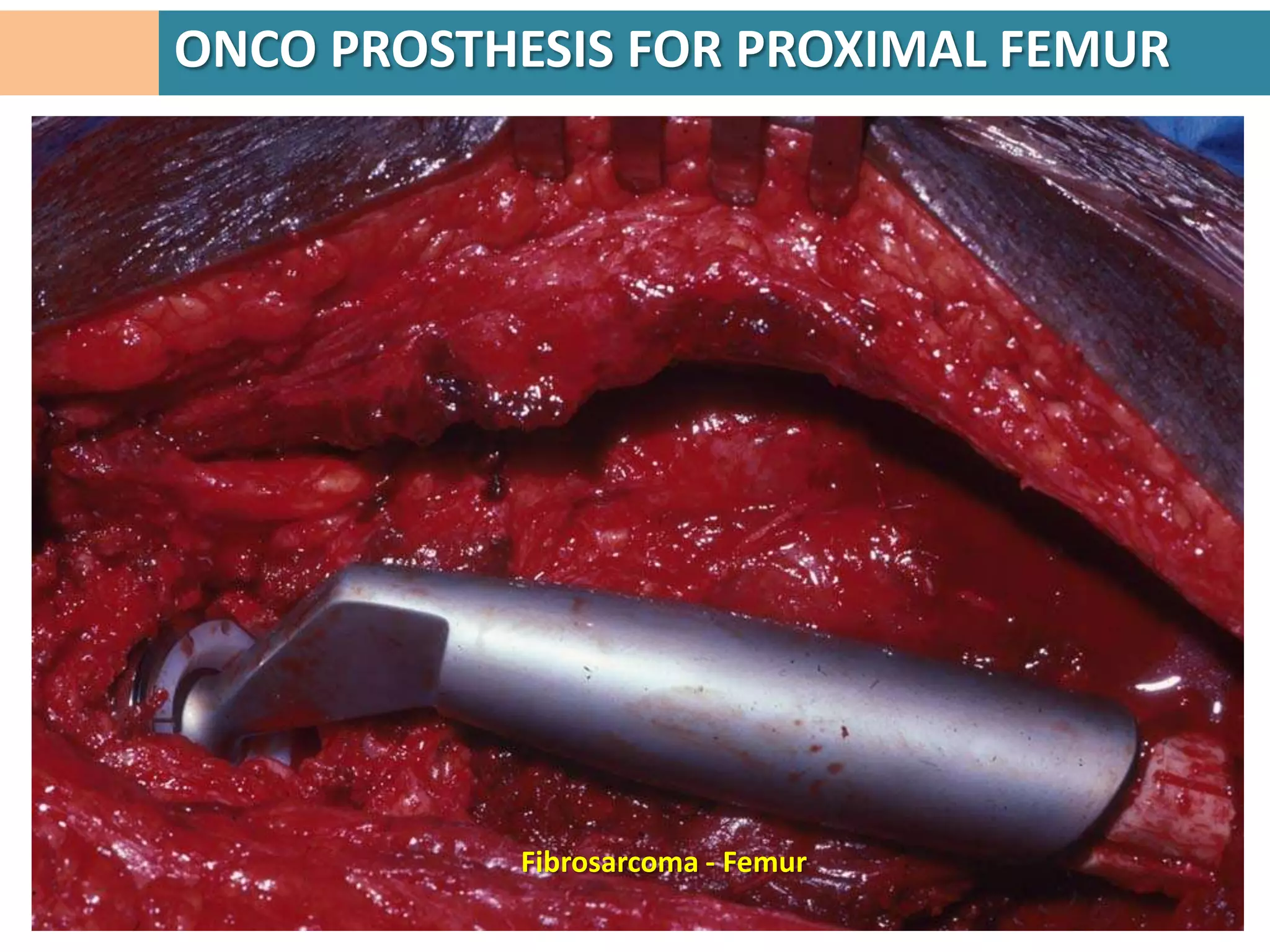
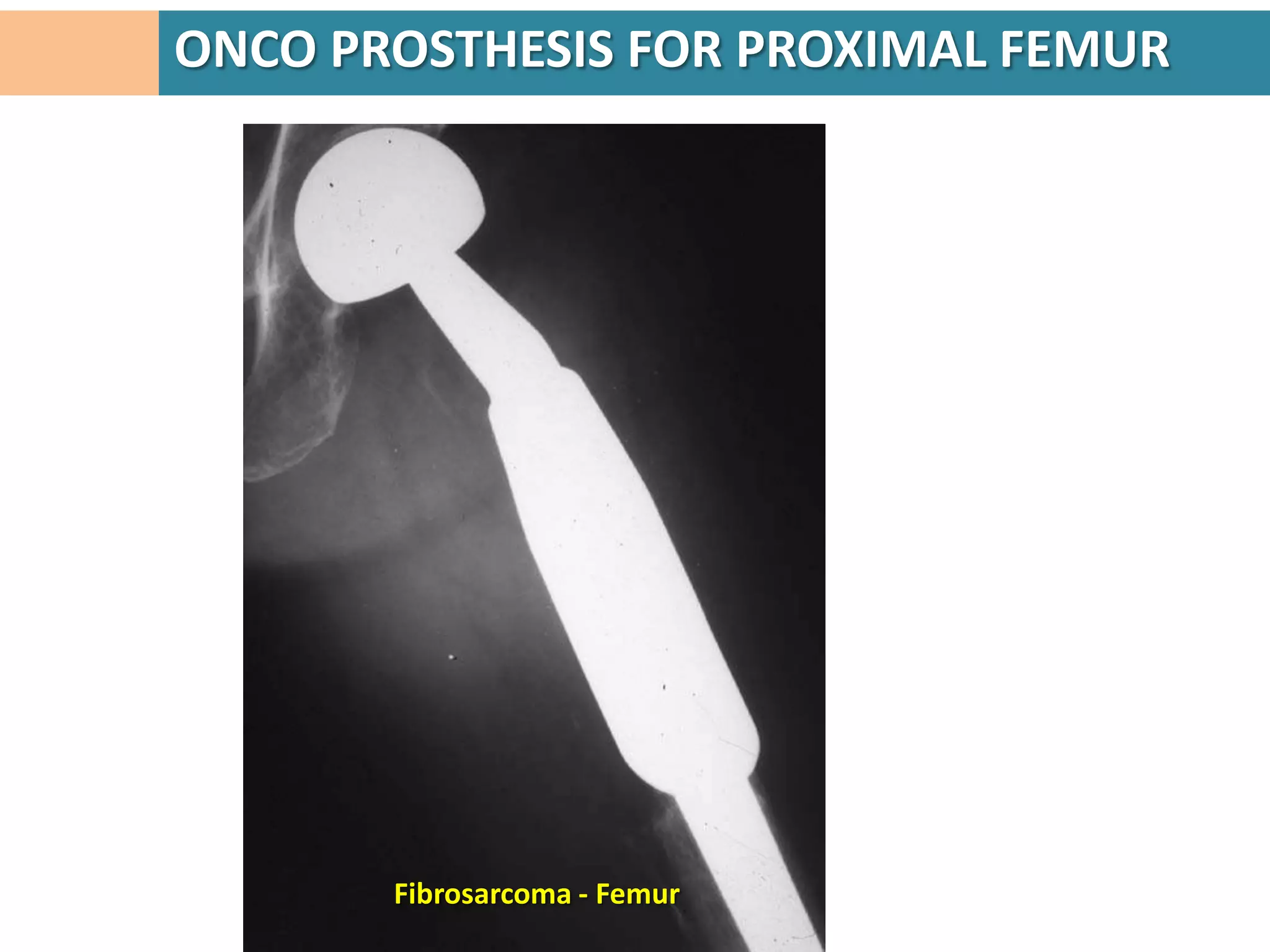
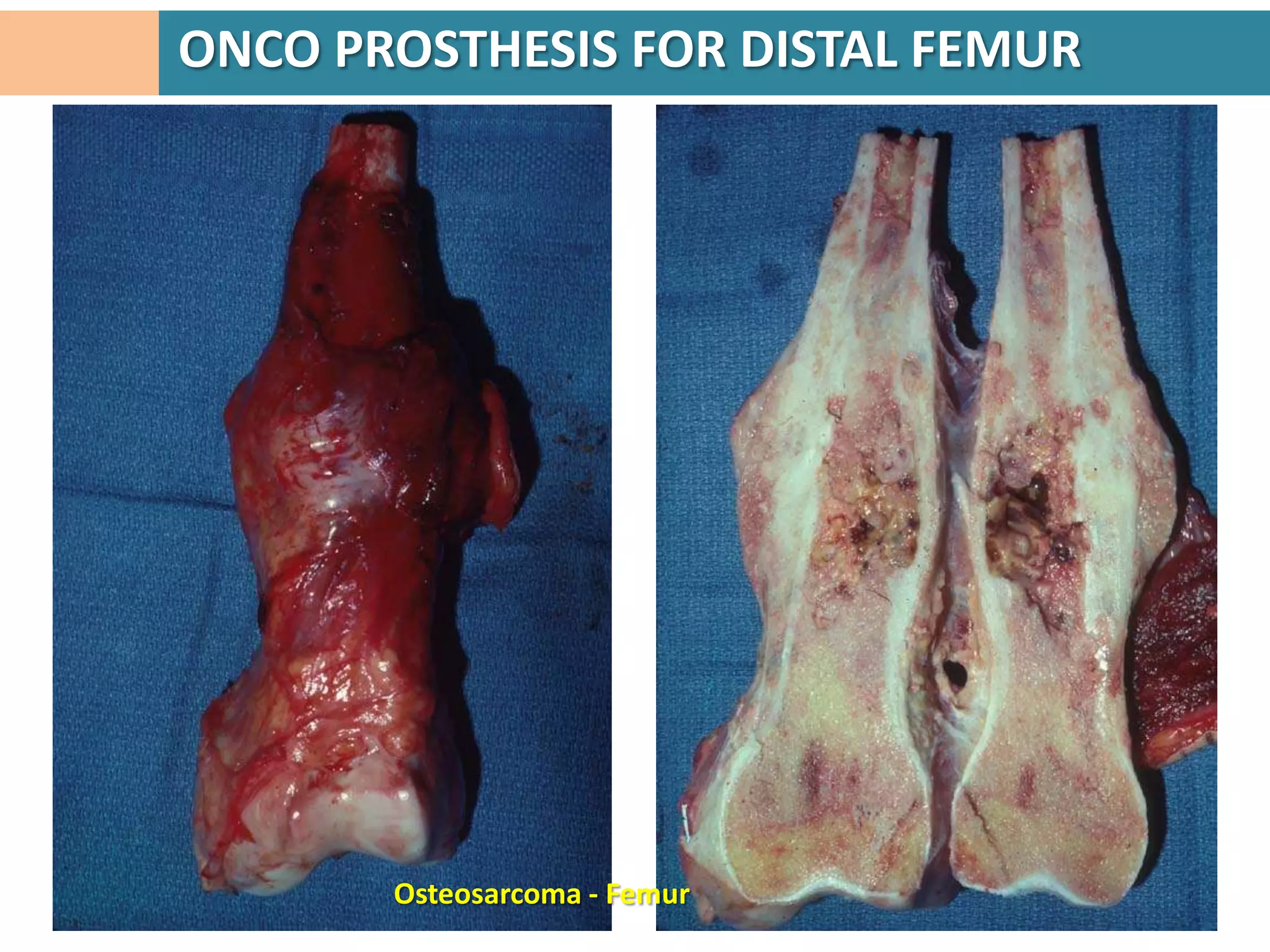
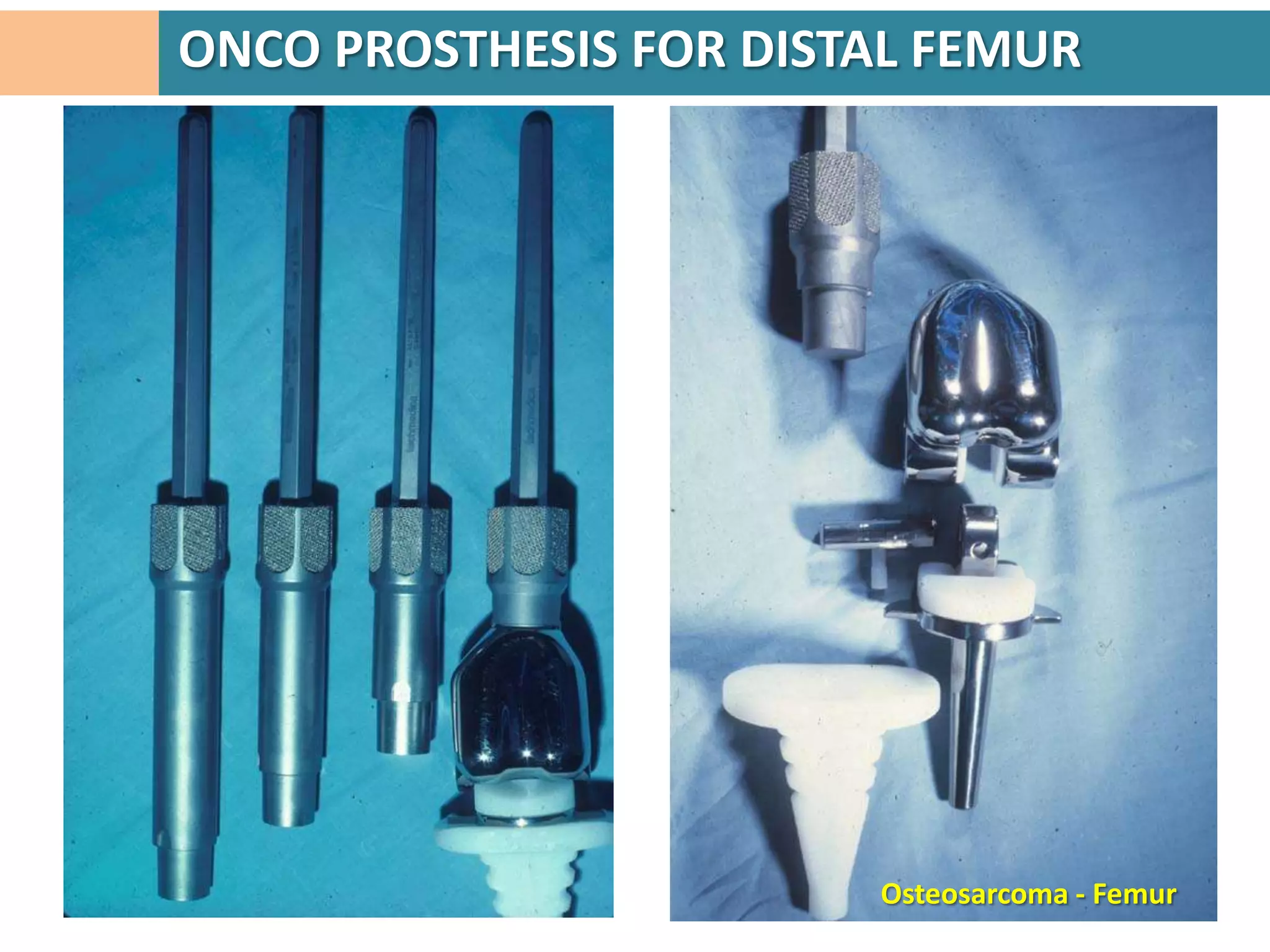
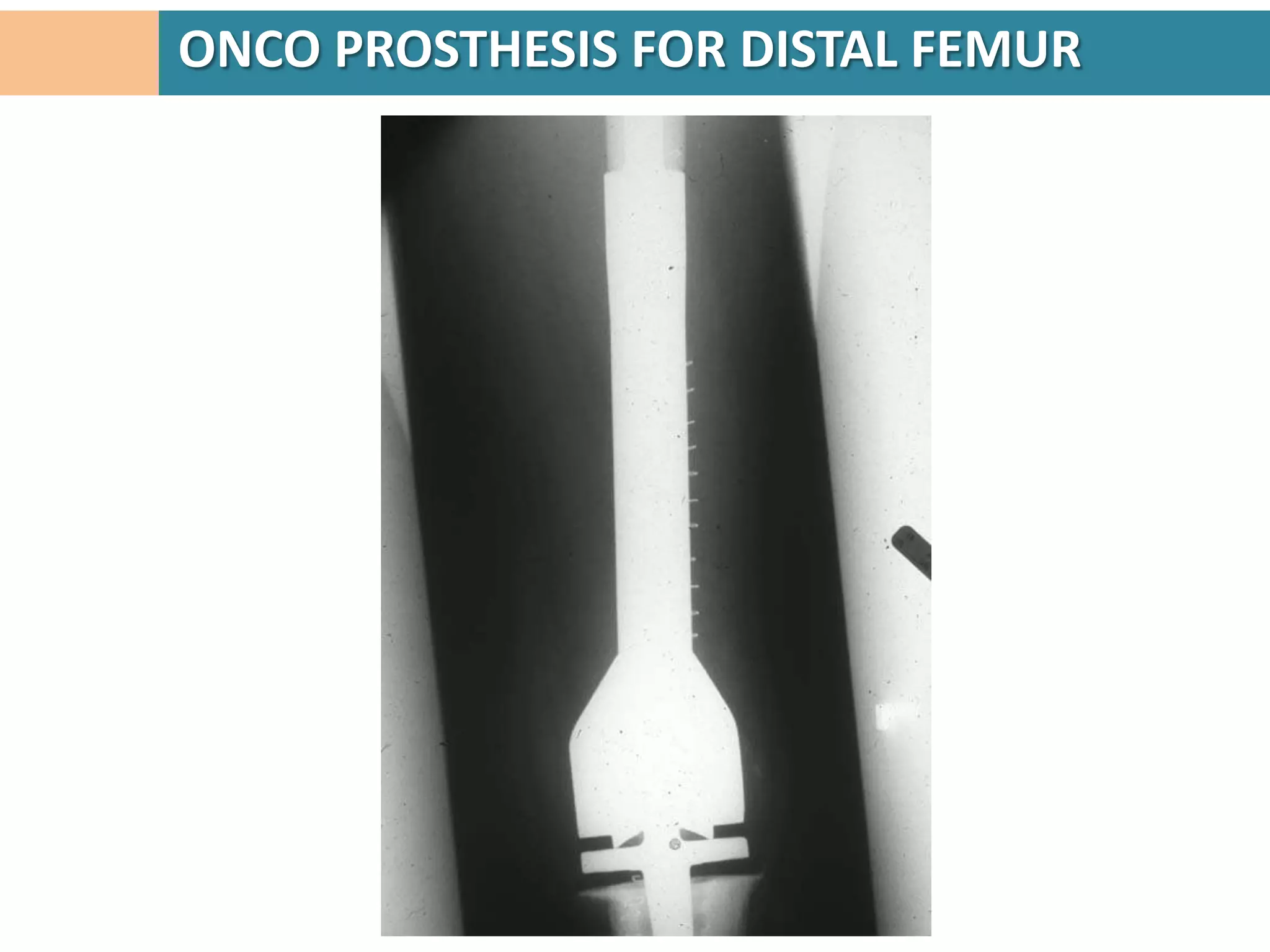
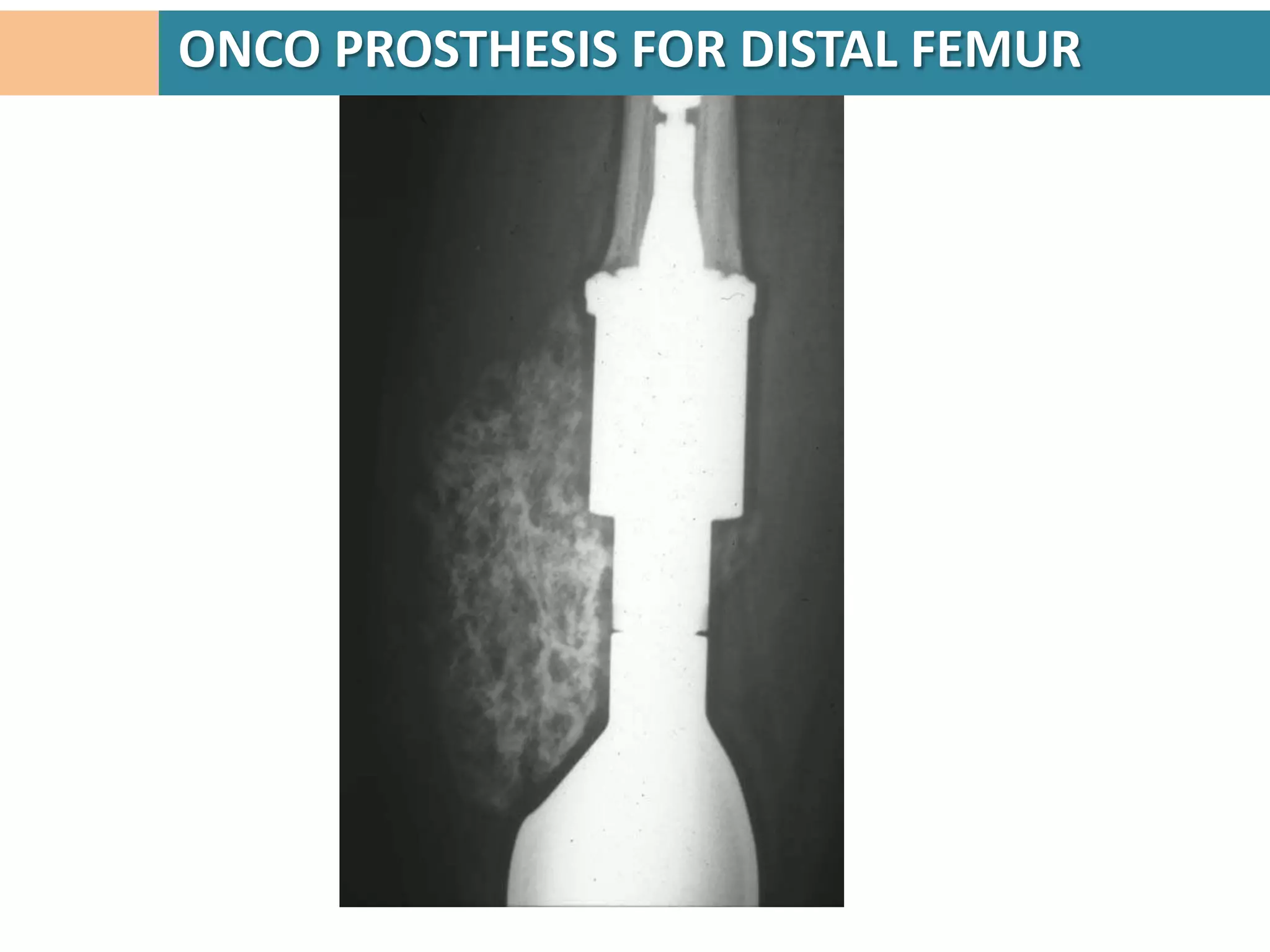
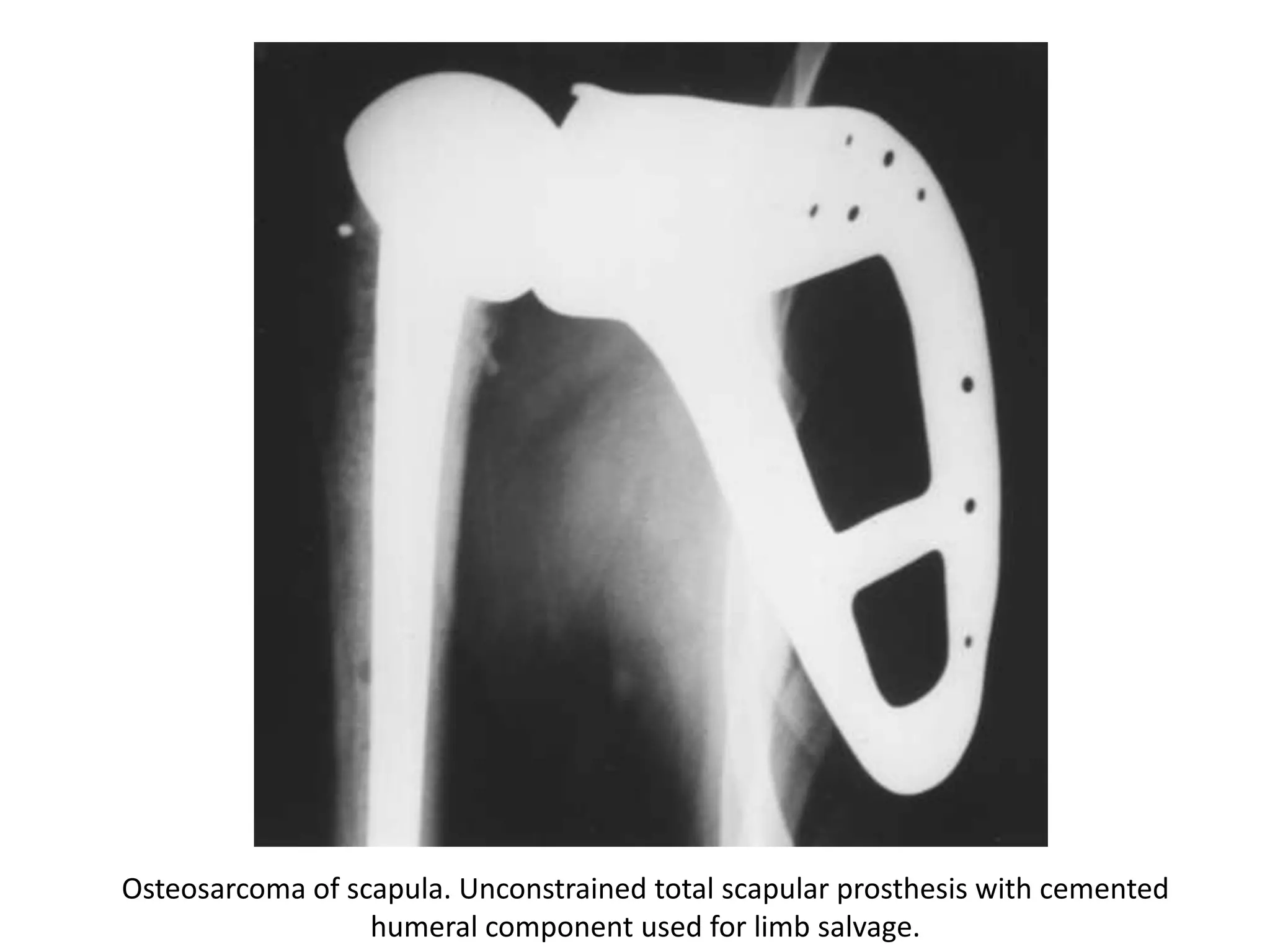
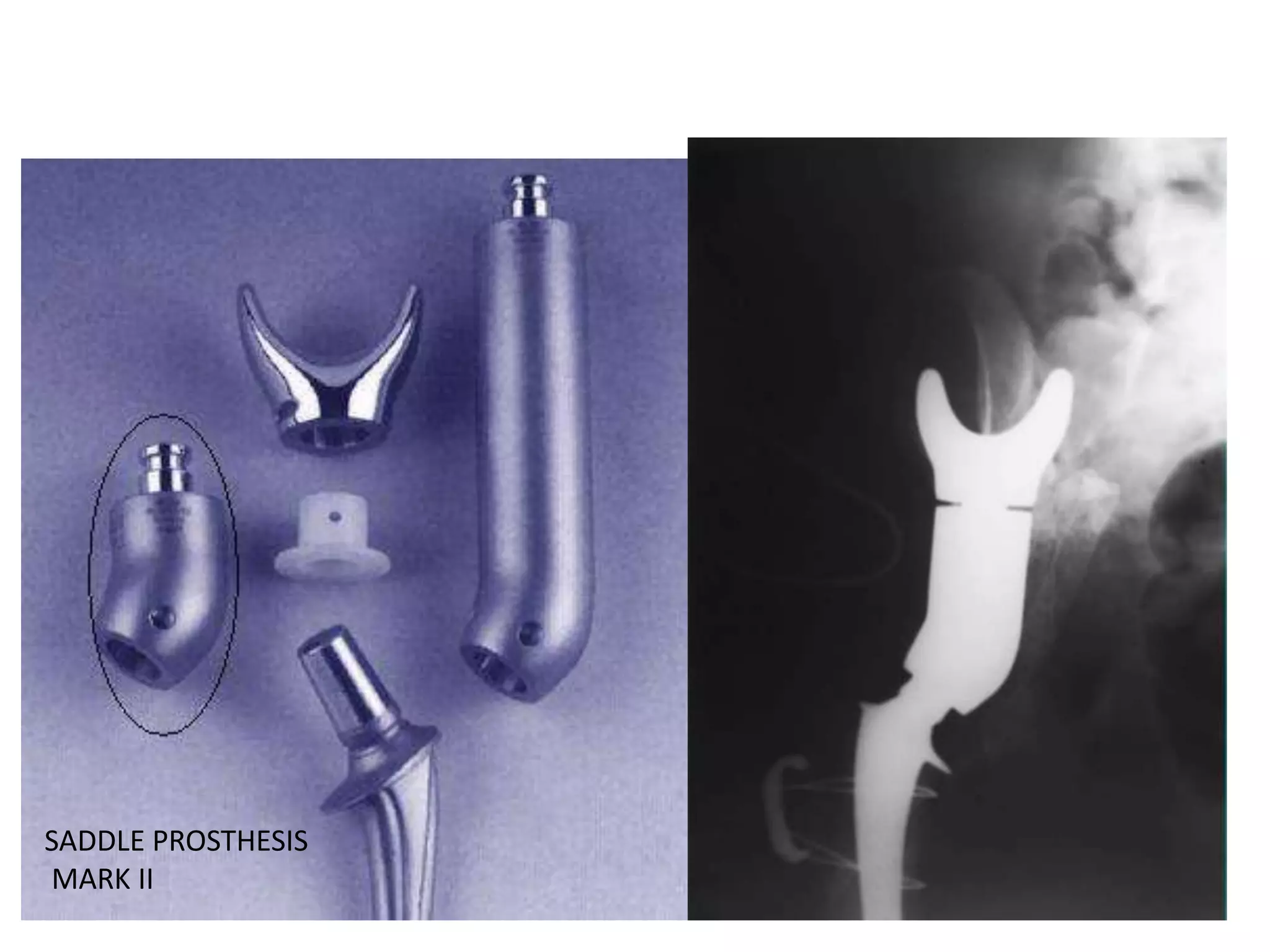
Advantages of allografts including incorporation into host tissue and better function post-surgery.Focus on prosthetic reconstruction techniques with notable outcomes for various limb salvage cases.
Utilization of composite grafts combining allografts and prosthetics for better function.
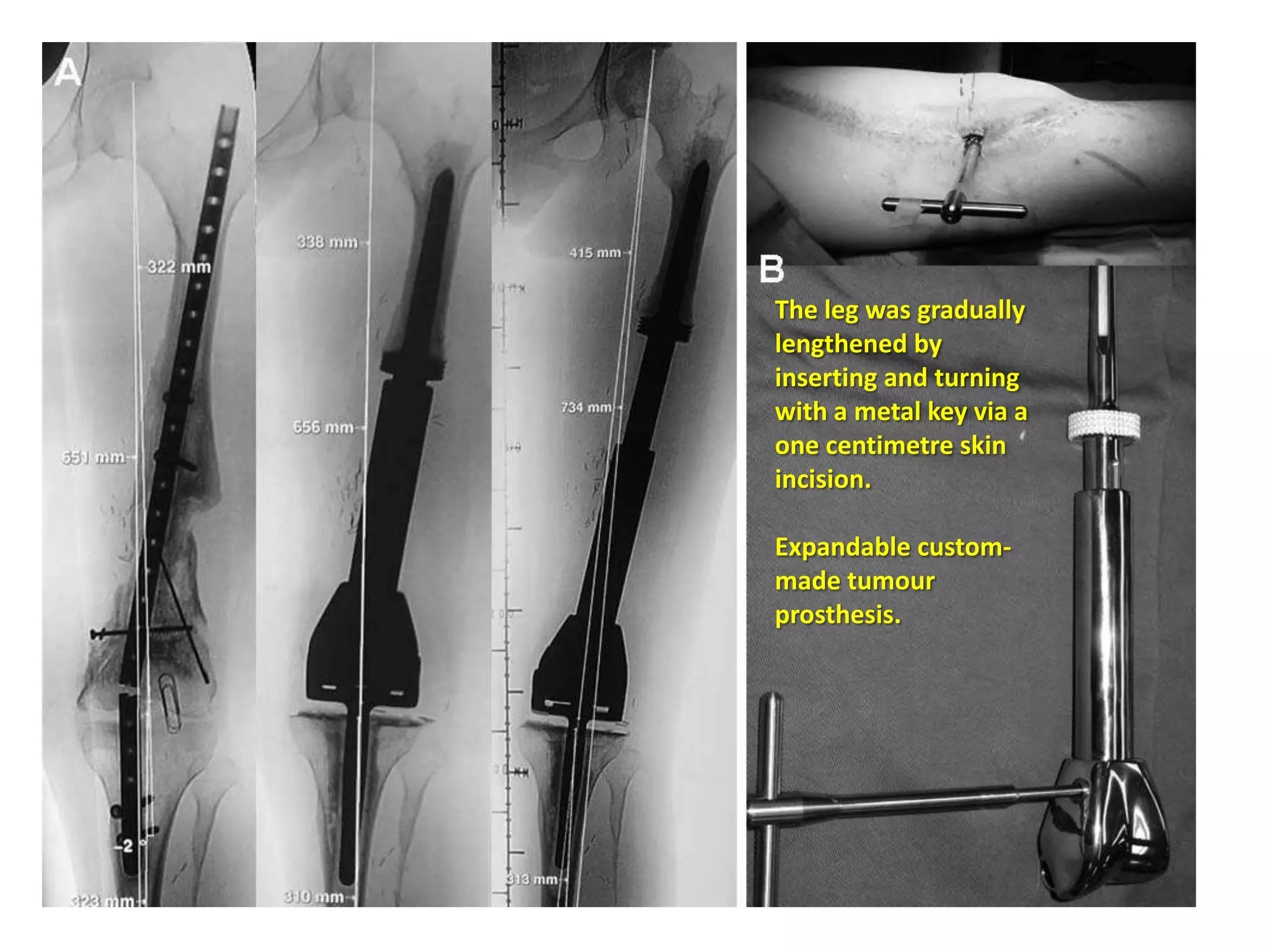
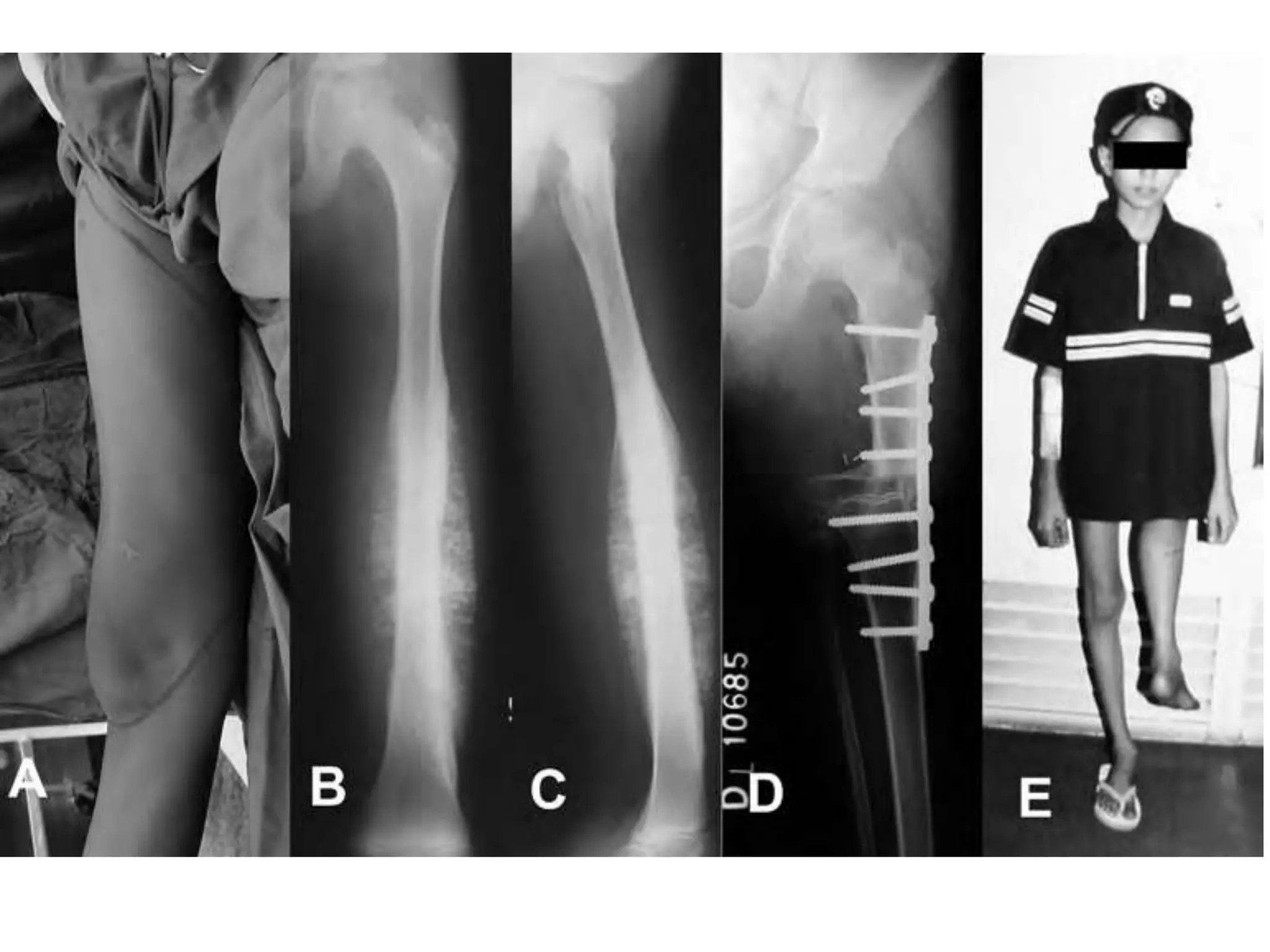
Specific strategies for limb salvage in children including biologic and non-biologic methods.
Presentation of clinical results, recurrence rates, and advances in limb salvage techniques.































































































