Downloaded 586 times
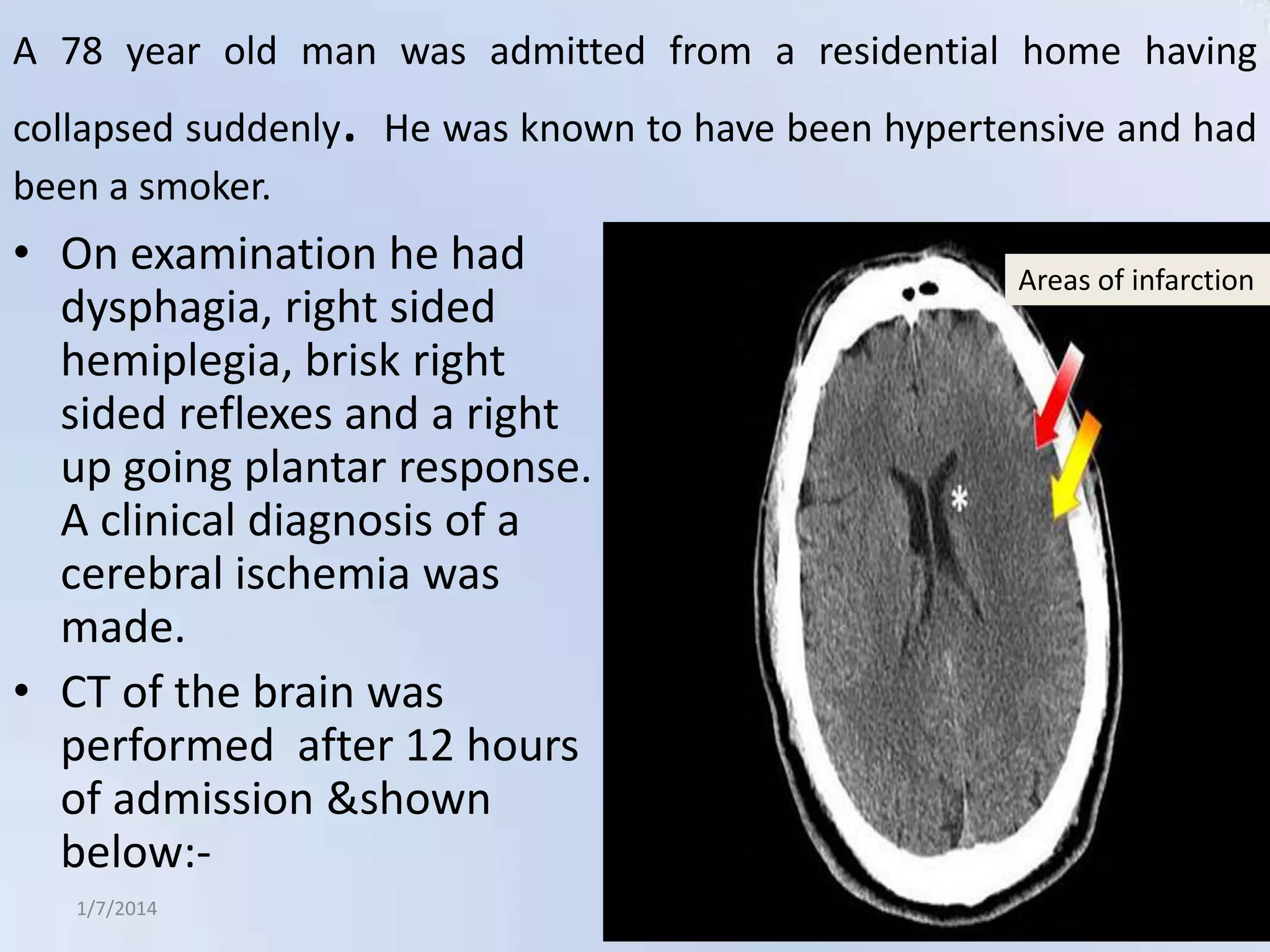


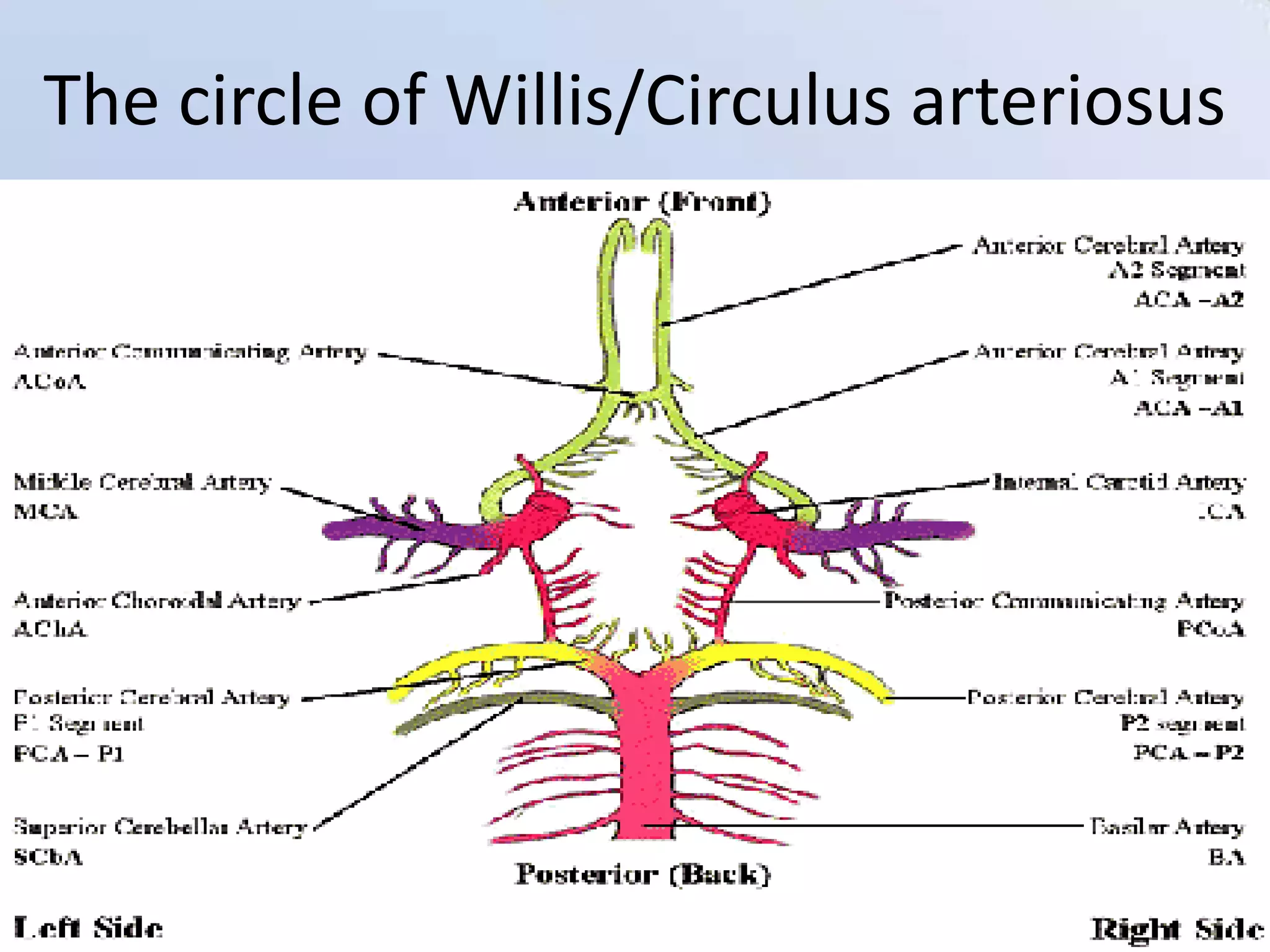




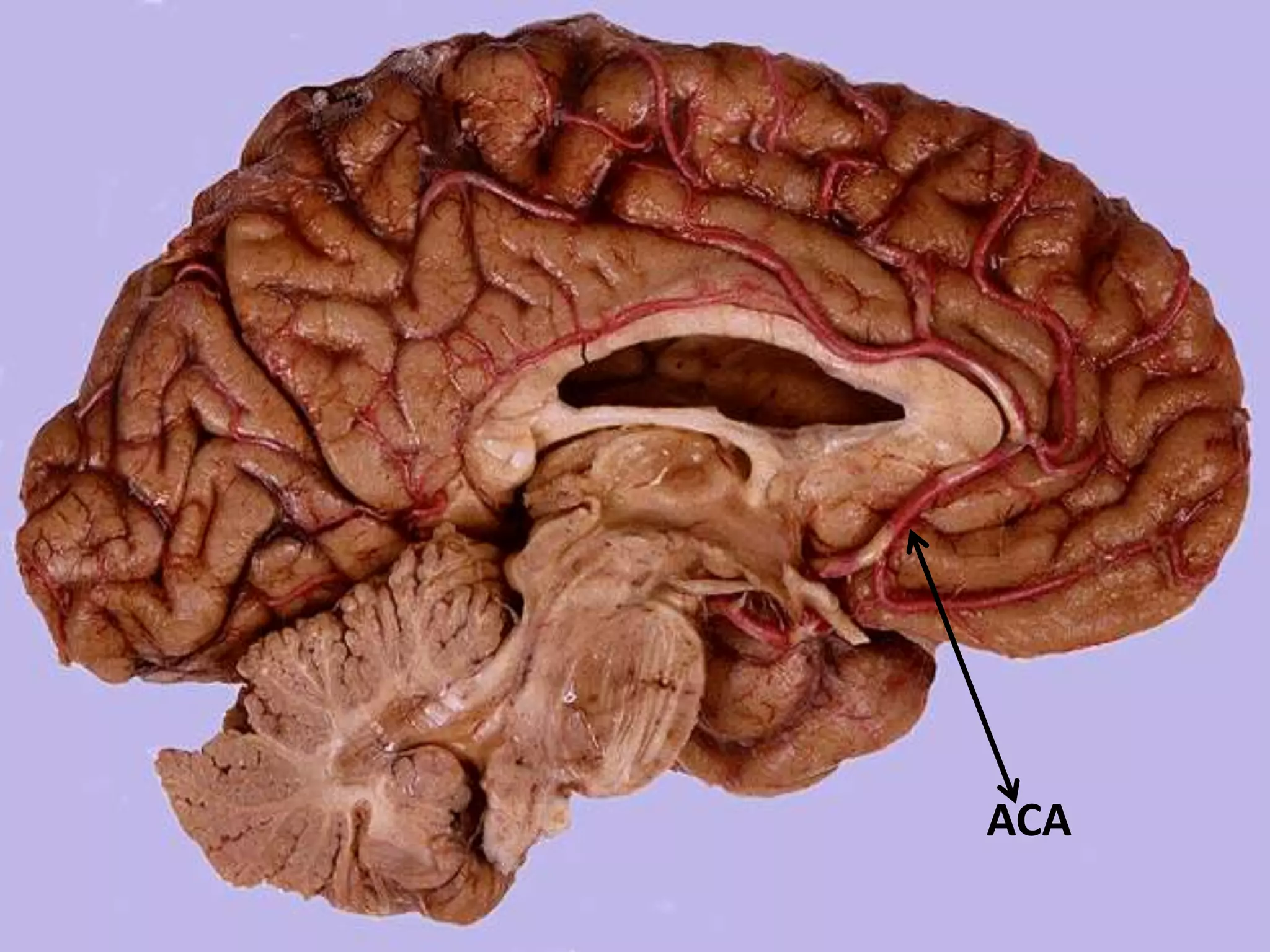



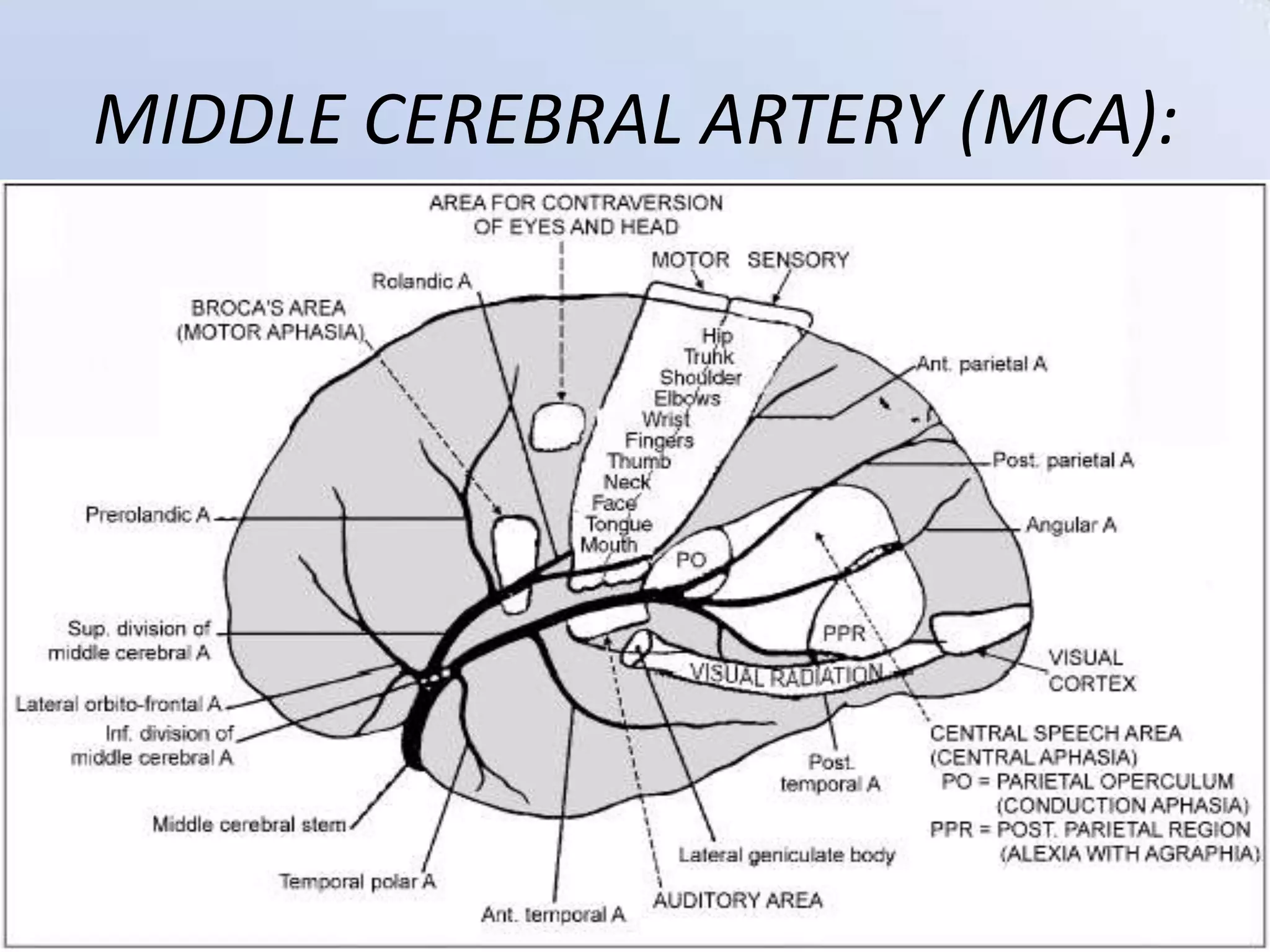


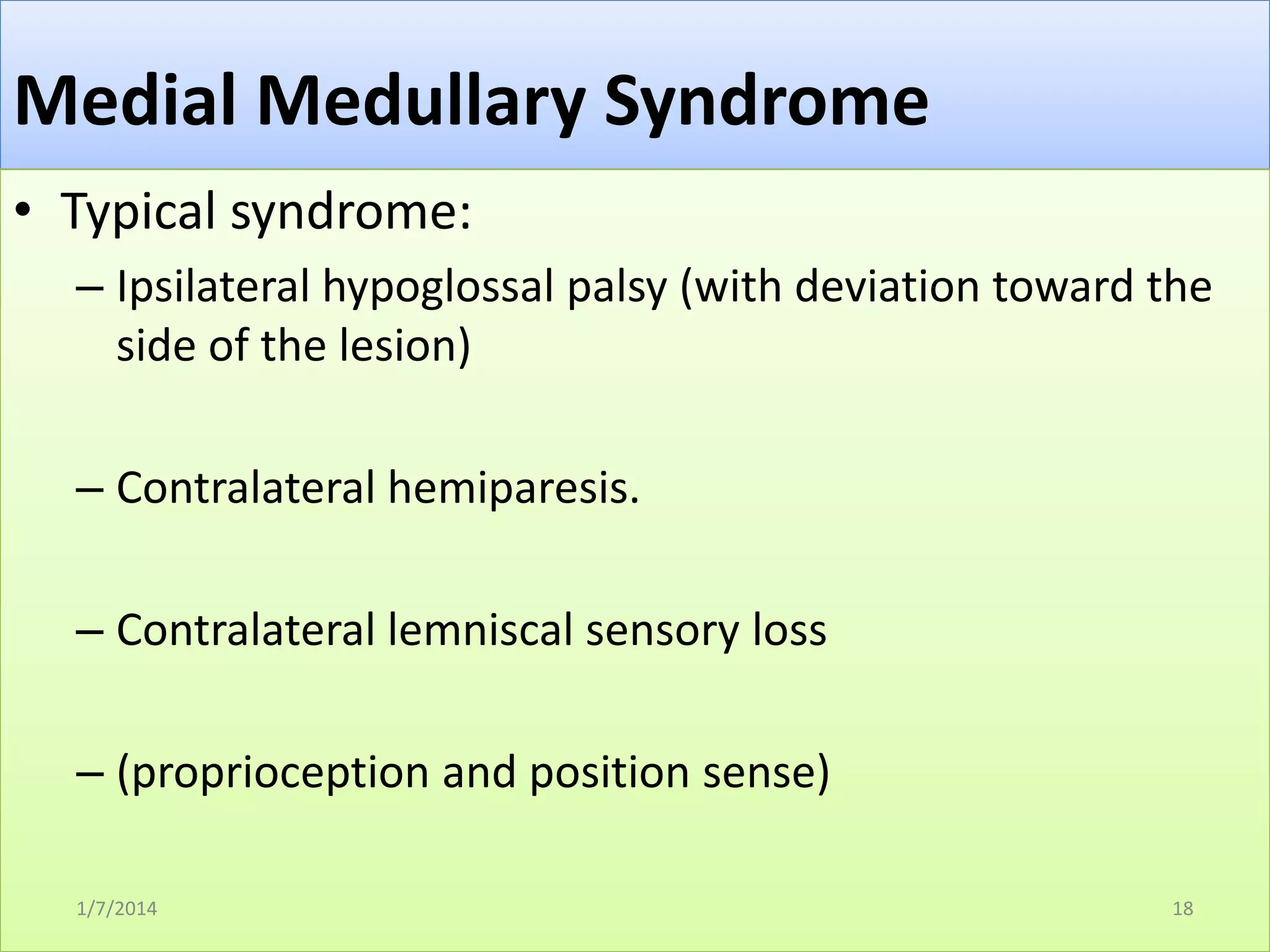


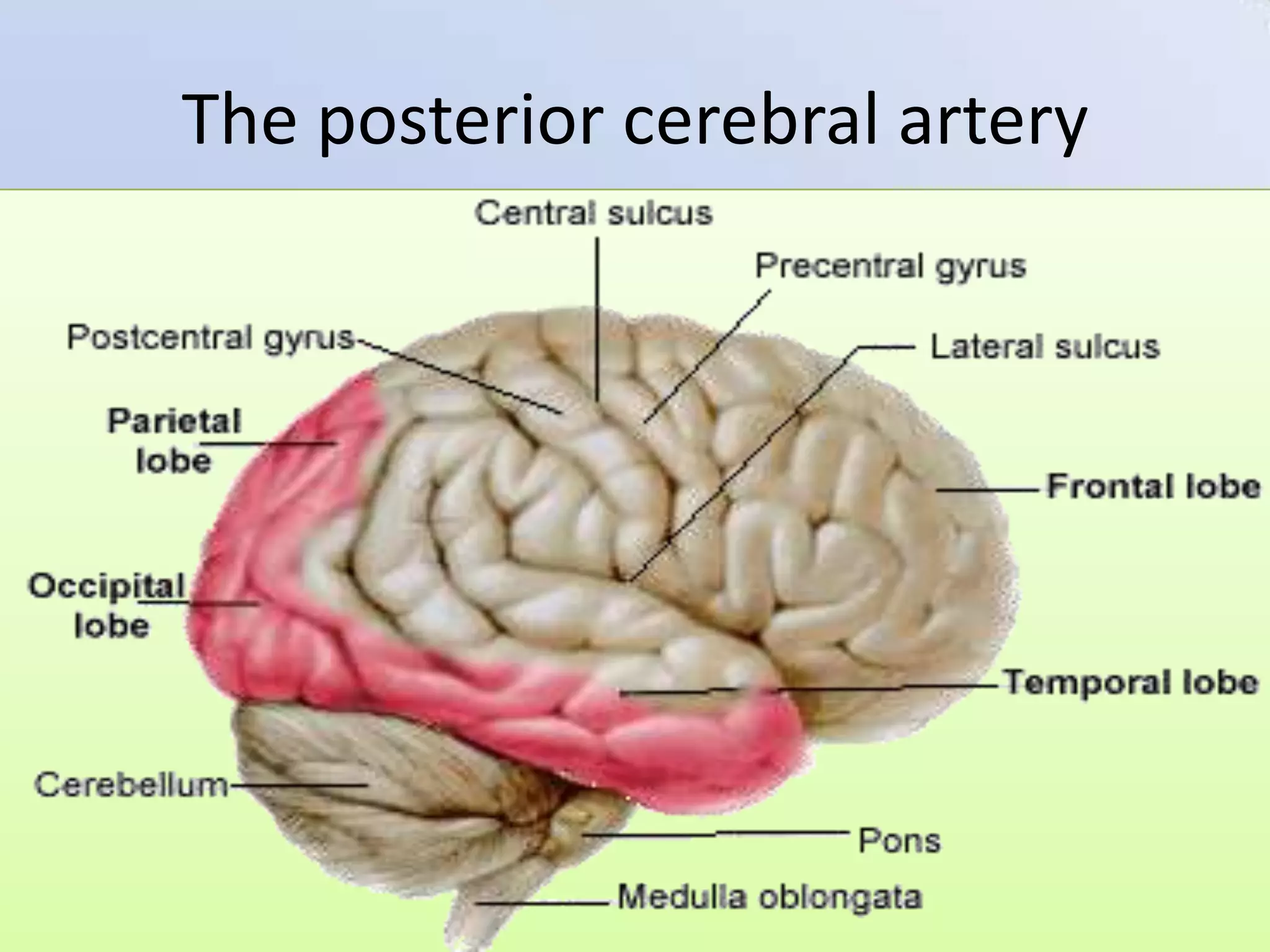
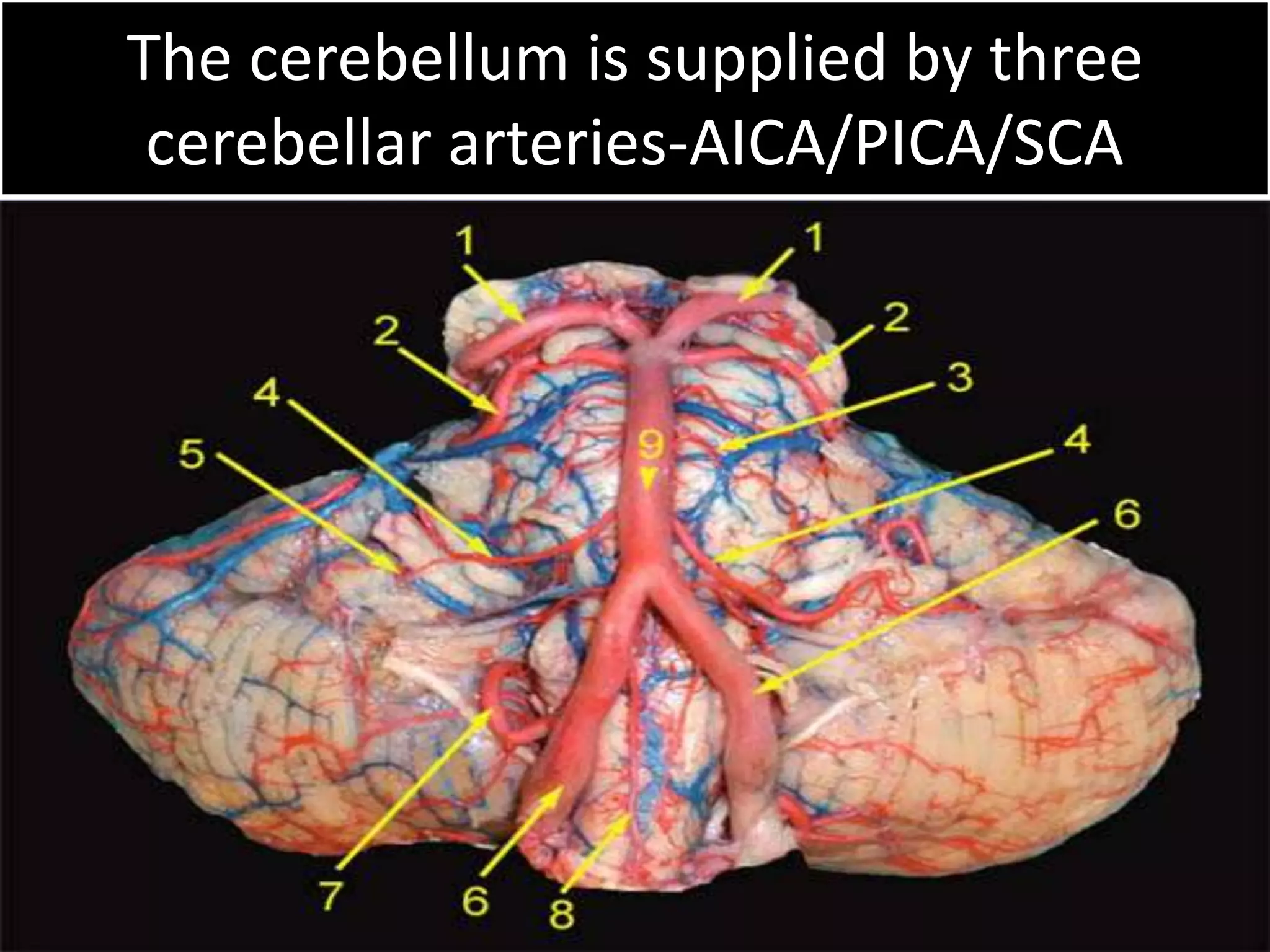
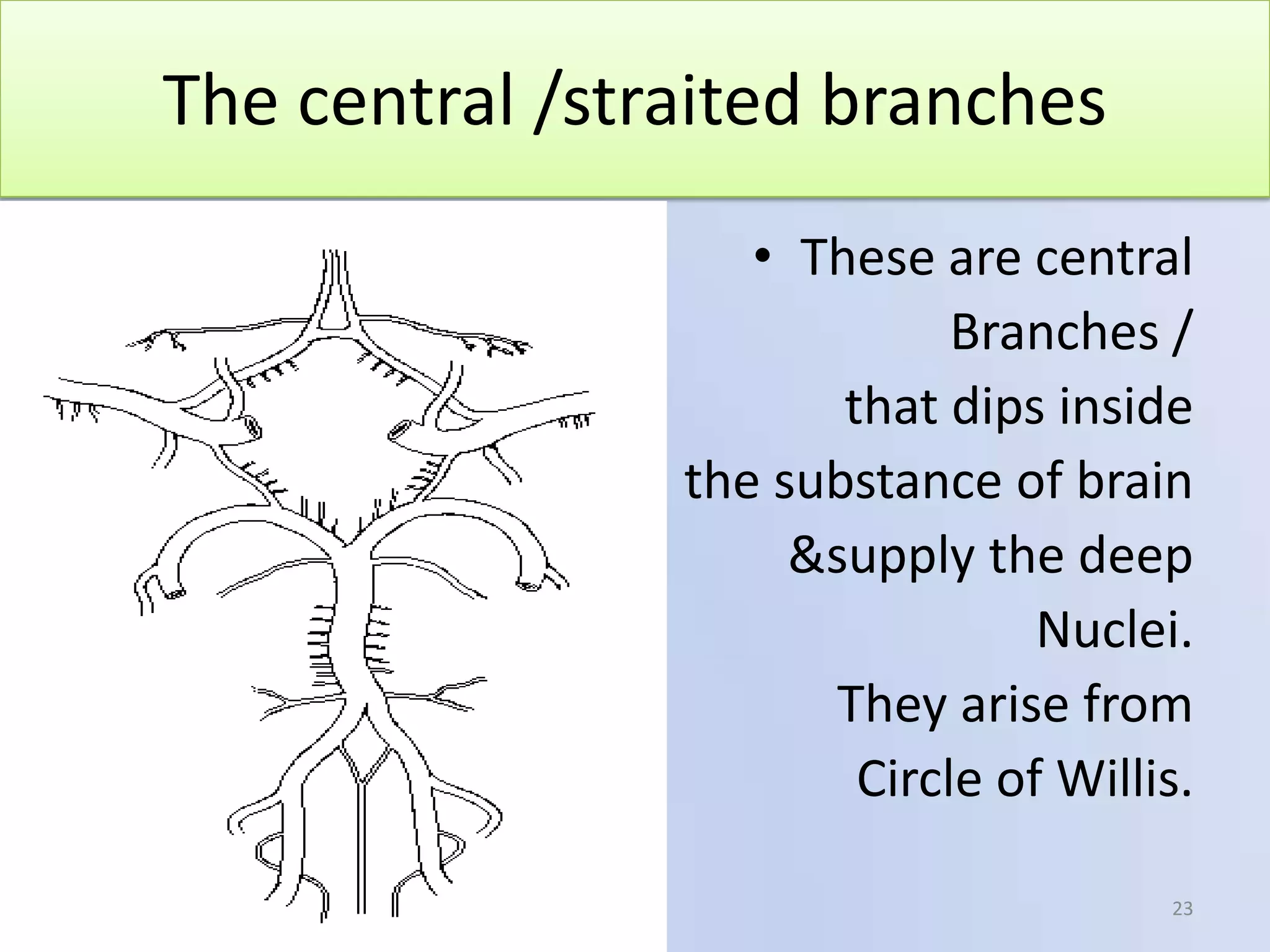




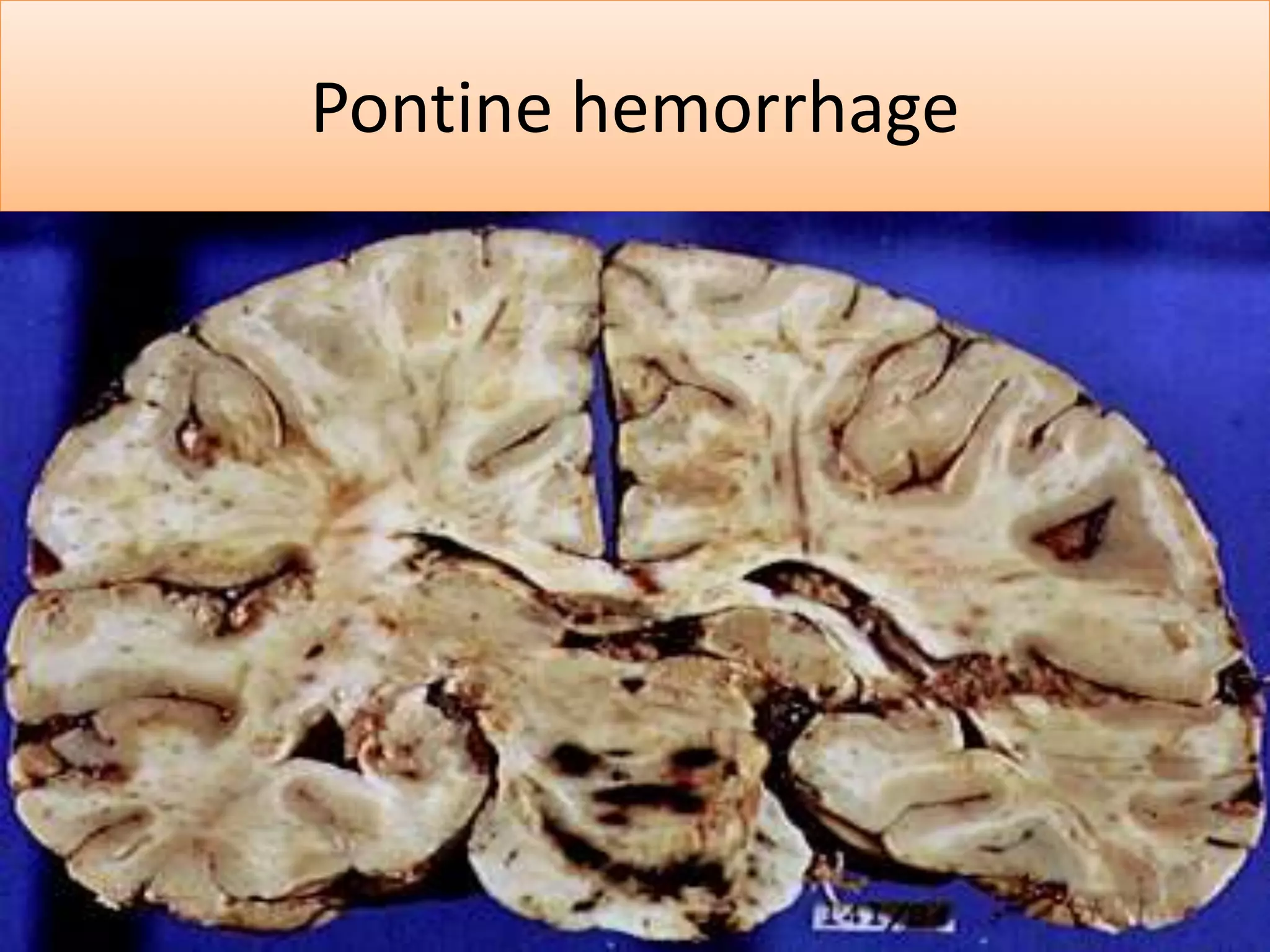




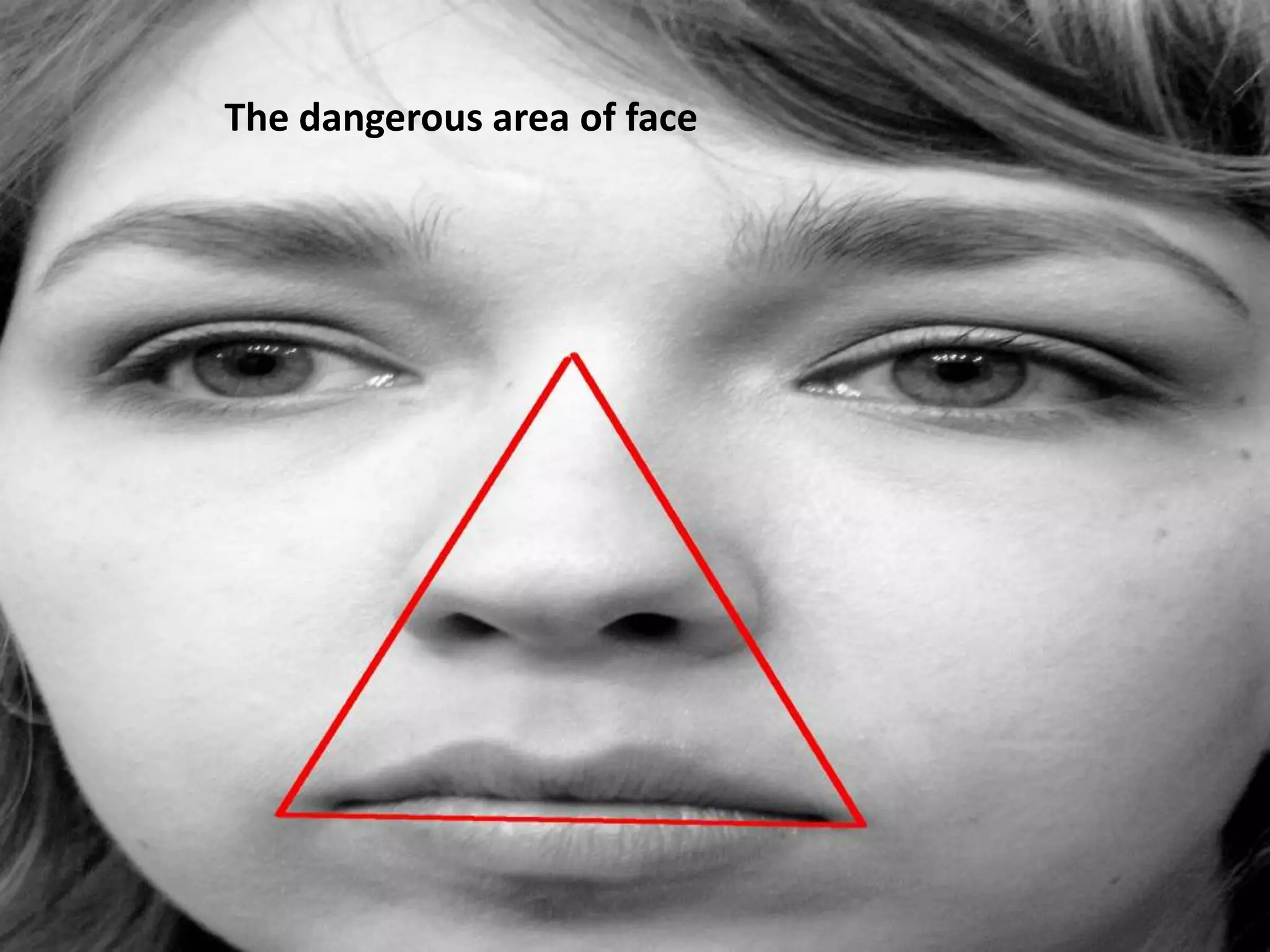
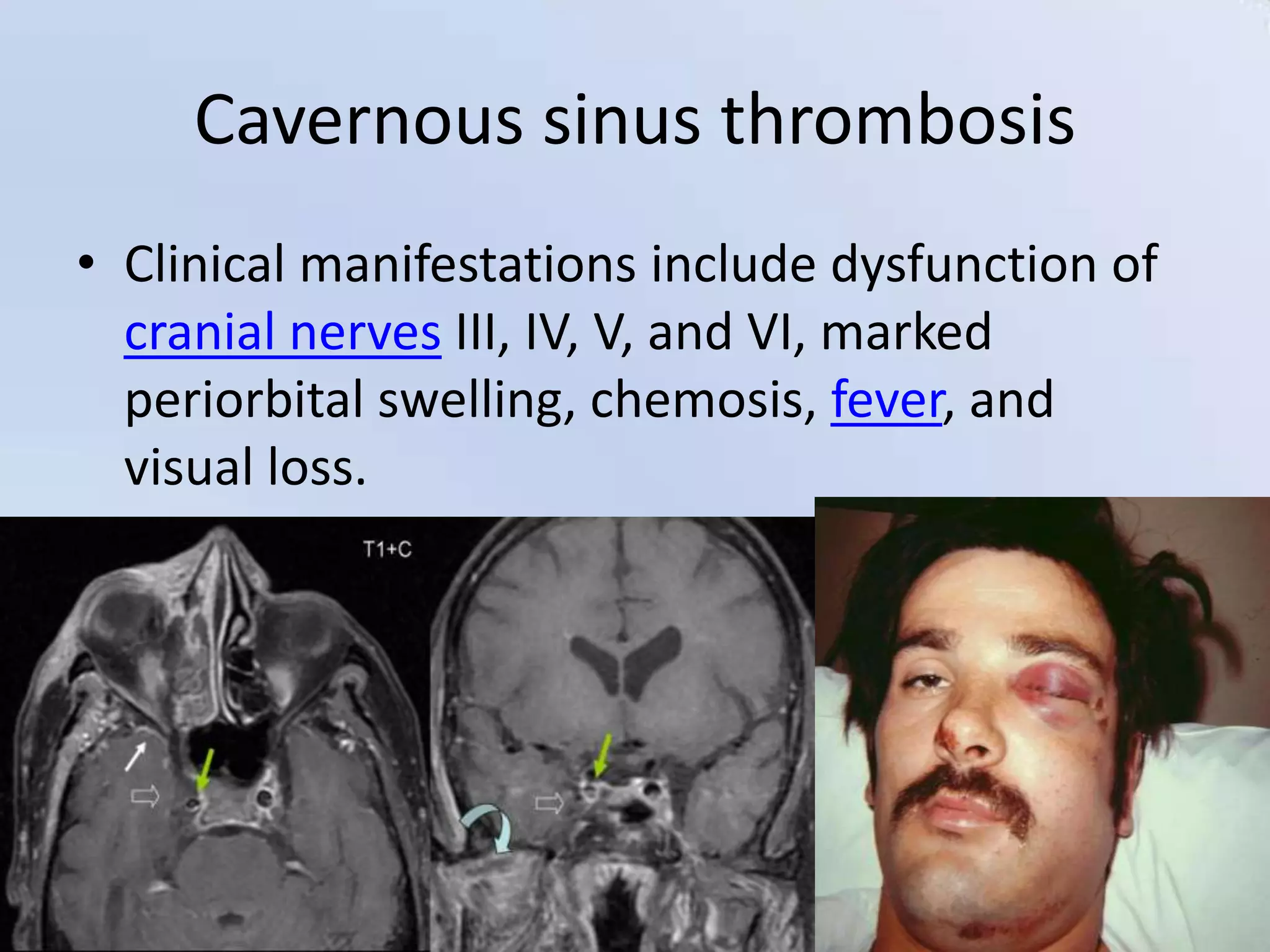

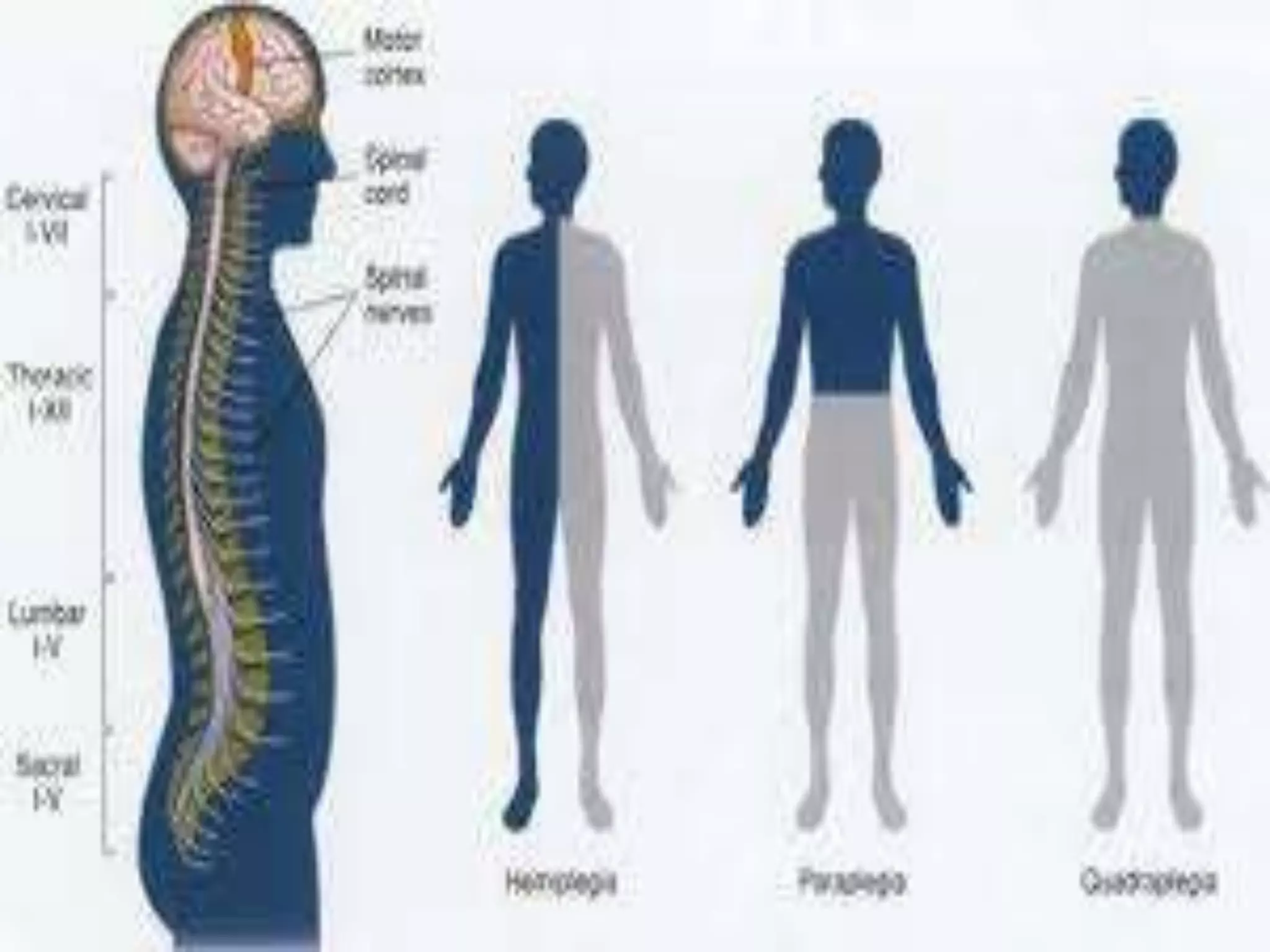

A 78-year-old man was admitted to the hospital after collapsing suddenly. He had a history of hypertension and smoking. Examination found right-sided weakness and abnormal reflexes, and CT scan showed areas of brain infarction. The document discusses the anatomy of the brain's blood supply through the circle of Willis and its branches, which areas of the brain each branch supplies, and clinical presentations that can result from occlusions or issues with different arteries like anterior cerebral artery occlusion causing paraplegia or middle cerebral artery occlusion causing face/arm weakness and neglect. It also covers venous drainage and conditions like cavernous sinus thrombosis.










































![Stroke [uncensored] - by MHR Corporation](https://cdn.slidesharecdn.com/ss_thumbnails/mhr4-stroke-101129110104-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)












































